BACKGROUND Prescription opioid overdoses are an ongoing public health concern across North America, contributing to more than 15,000 deaths in the United States in 2015.
BACKGROUND Prescription opioid overdoses are an ongoing public health concern across North America, contributing to more than 15,000 deaths in the United States in 2015.
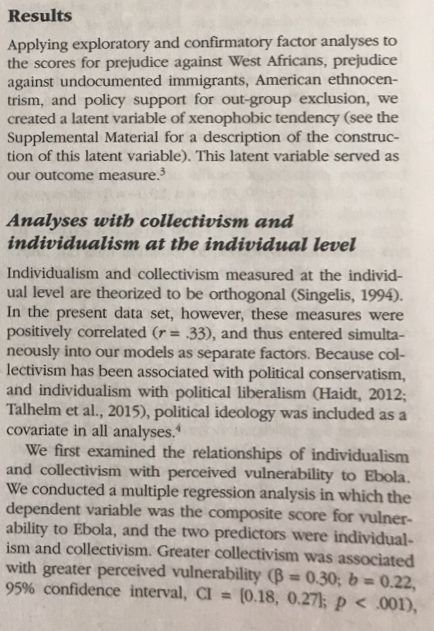
BACKGROUND Prescription opioid overdoses are an ongoing public health concern across North America, contributing to more than 15,030 deaths in the United States in 2015 [1]. Most opioidrelated deaths result from respiratory depression, and coadministration of central nervous system {CNS} depressants is an important and avoidable risk factorfor death. Recent evidence showed that co prescription of benzodiazepines with opioids increases the risk of overdose death nearly 4fold [2], leading to the introduction of black box warnings on the packaging for both products in August 2316 [3]. Furthermore, prescription opioid use has been shown to be highly associated with future risk of opioidrelated death, with 1 of every 550 chronic opioid users dying within approximately 2.5 years of theirfirst opioid prescription [4]. Gabapentin is an anticonvulsant commonly used as an adjunct forthe treatment of chronic pain [5]. Although gabapentin is widely perceived as safe [5,5], drug-induced respiratory depression has been described when gabapentin is used alone or in combination with other medications [ii10]. Indeed, the product monograph was amended in 2014 to warn about possible respiratory depression when combined with opioids [11]. Potential risk factors for gabapentin related respiratory depression include advancing age, renal insufficiency, chronic lung disease, and dose. The role of dose is particularly important in light of data indicating a 44% increase in systemic gabapentin exposure following its administration with morphine [81CI,12,13], likely reflecting increased drug absorption from lowered intestinal motility [12]. Because gabapentin and opioids are both commonly prescribed for pain, the likelihood of coprescription is high [1412]. However, to our knowledge, no published studies have examined whether concomitant gabapentin therapy is associated with an increased risk of accidental opioidrelated death in patients receiving opioids. We hypothesized that individuals coprescribed opioids and gabapentin would have a higher risk of opioidrelated death, and that there would be a doseresponse gradient with increasing gabapentin dose. METHODS Setting: We conducted a populationbased casecontrol study of adults dispensed opioid analgesics underthe Ontario Public Drug Programs between August 1, 199?, and December 31, 2013. All residents of Ontario receive publicly funded physician and hospital care. Public drug coverage for prescription medications is provided to individuals aged 65 years and older, as well as those who are unemployed, are receiving disability benefits, have high drug costs relative to their net household income, are receiving home care services, or reside in a longterm care home. The study protocol was approved by the research ethics board of Sun nyb rook Health Sciences Centre, Toronto, Ontario. Data sources: We used the Ontario Drug Benefit {ODE} database to identify prescription medications dispensed to eligible residents of Ontario overthe study period. We abstracted detailed information on confirmed opioidrelated deaths from the Office of the Chief Coroner of Ontario using methods described previously [ED]. Identification of patients and outcomes: We identified a cohort of ODB- eligible individuals aged 15 to 1135 years who were treated with at least 1 opioid prescription over the study period, including oral formulations of morphine, codeine, oxycodone, meperidine, and hydromorphone, as well as transdermal fentanyl patches. We excluded prescriptions for rarely used opioids {such as pentazocine or anileridine}, parenteral or intranasal opioid formulations, and methadone, which in Ontario is principally used to treat opioid use disorders. We defined cases as individuals who died from an opioid-related cause overthe study period, and excluded opioid overdoses deemed to be suicides or homicides by the investigating coroner. We defined the index date as the date of death. The index date {date of death} for potential controls was randomly assigned according to the distribution of index dates {date of death} for included cases. We excluded individuals with invalid identifiers and those with a prior diagnosis of cancer or evidence of palliative care in the 6 months preceding the index date. Consequently, our analyses were limited to patients receiving opioids for noncancer pain. We required that all study patients have at least 1 opioid prescription overlapping with their index date {date of death}, and at least 6 months of continuous eligibility for public drug benefits priorto their index date {date of death]. We matched each case with up to 4 controls on their disease risk. index {within 0.2 standard deviations}, age {within 5 years}, sex, year of index date {within 1 year}, and history of chronic kidney disease {prior 5 years}. When a full number of matches could not be found, we matched as many controls as possible to each case, and any available clinical practice. Our study has important implications. for public health, particularly given the high degree of coprescription. Almost 10% of patients treated with an opioid in our study also used gabapentin, while nearly half of patients treated with gabapentin were coprescribed opioids. Similarly, studies from the United States and United Kingdom have estimated that between 15% and 22% of people with opioid use disorder are also misusing gabapentin [17]. Gabapentin is frequently used as an adjunct to opioids for neuropathic pain syndromes, but physicians may not be aware of the potential for respiratory depression with this drug; thus, increased awareness among patients and clinicians about the potential fora lifethreatening interaction between these drugs is essential. When coprescription is necessary, strategies for minimizing the seguelae of this interaction should be considered, including cautious dose titration, dose adjustment in the setting of comorbid lung and kidney disease, and avoidance of other CNS depressants. In addition, patients treated with this combination should be instructed to seek medical attention immediately if symptoms of opioid overdose occur. Finally, because of pregabalin's pharmacologic similarities to gabapentin, it is possible that pregabalin imparts a similar risk of overdose and death among opioid users, a hypothesis supported in part by cases of respiratory depression associated with this drug [28]. CONCLUSION In this study we found that, among patients prescribed opioids, co-prescription of gabapentin was associated with a considerable increase in the risk of opioid-related death, particularly at higher doses. The clinical consequences ofa potential drugdrug interaction are clear given the large number of people at risk of this fatal outcome. Clinicians should consider carefully whetherto continue prescribing this combination of products and, when coprescription is deemed necessary, should closely monitortheir patients and adjust opioid dose accordingly. Future research should investigate whether a similar interaction exists between pregabalin and opioids. OUESTIONS 1E}. 1'u'y'hat are the conclusions? [13 pts.} Results: Try not to get frustrated with all the numbers, just focus on the main statements found in the results. You are not expected to know how to read the statistics here. Graphs / Figures also help. 8) They said they first examined the relationship between individualism and collectivism to perceived vulnerability to Ebola. What was the first finding they discovered on page 938? 9) What does Figure 1a show? What was the finding? 10) What does Figure 1b show? What was the finding?Results Applying exploratory and confirmatory factor analyses to the scores for prejudice against West Africans, prejudice against undocumented immigrants, American ethnocen- trism, and policy support for out-group exclusion, we created a latent variable of xenophobic tendency (see the Supplemental Material for a description of the construc tion of this latent variable). This latent variable served as our outcome measure. Analyses with collectivism and individualism at the individual level Individualism and collectivism measured at the individ- ual level are theorized to be orthogonal (Singelis, 1994). In the present data set, however, these measures were positively correlated (r = .33), and thus entered simulta neously into our models as separate factors. Because col- lectivism has been associated with political conservatism, and individualism with political liberalism CHaidt, 2012; Talhelm et al., 2015), political ideology was included as a covariate in all analyses.* We first examined the relationships of individualism and collectivism with perceived vulnerability to Ebola. We conducted a multiple regression analysis in which the dependent variable was the composite score for vulner- ability to Ebola, and the two predictors were individual- ism and collectivism. Greater collectivism was associated with greater perceived vulnerability (B = 0.30; b = 0.22, 95% confidence interval, CI = [0.18, 0.27); p
Step by Step Solution
There are 3 Steps involved in it
Step: 1
Get Instant Access to Expert-Tailored Solutions
See step-by-step solutions with expert insights and AI powered tools for academic success
Step: 2
Step: 3
Ace Your Homework with AI
Get the answers you need in no time with our AI-driven, step-by-step assistance