

 \
\
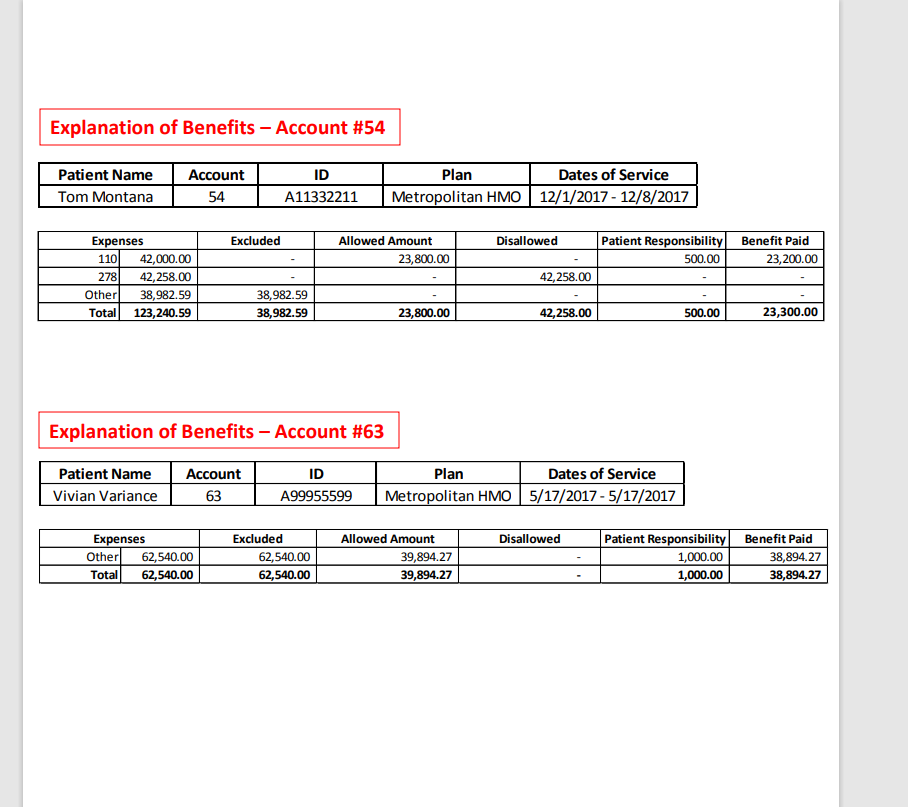
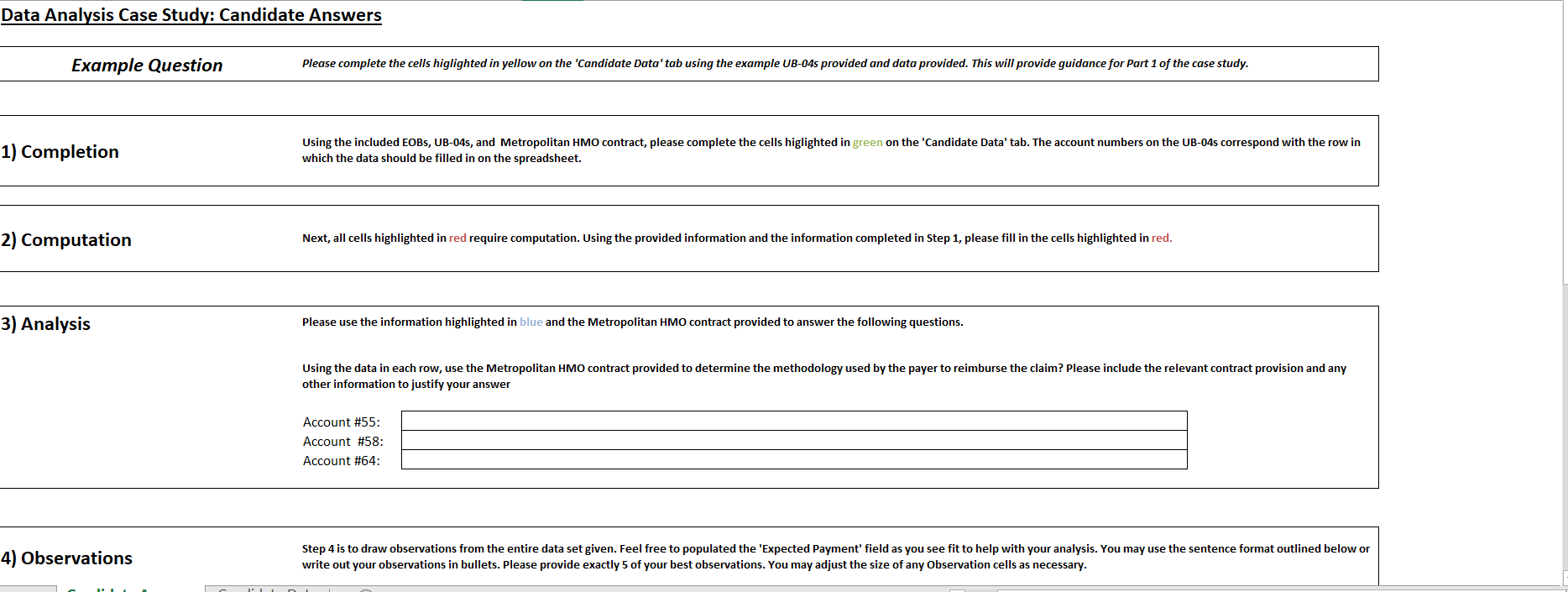
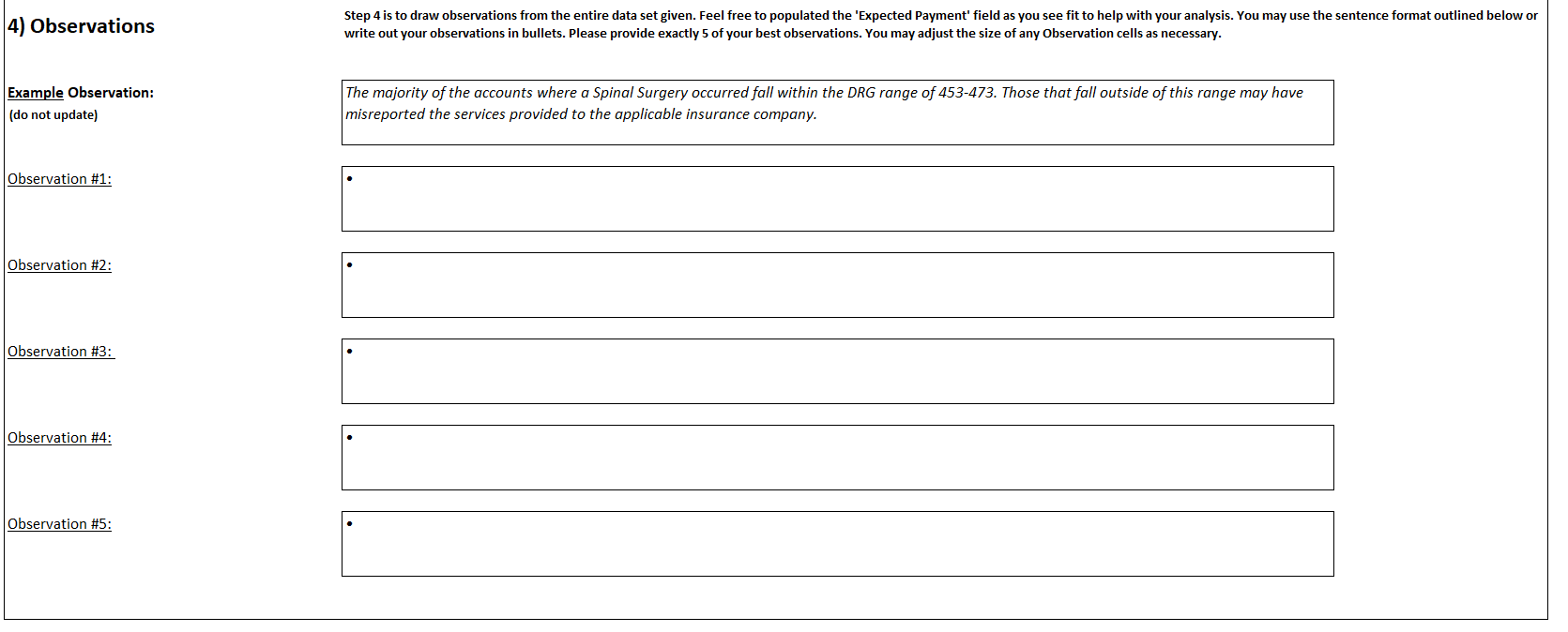
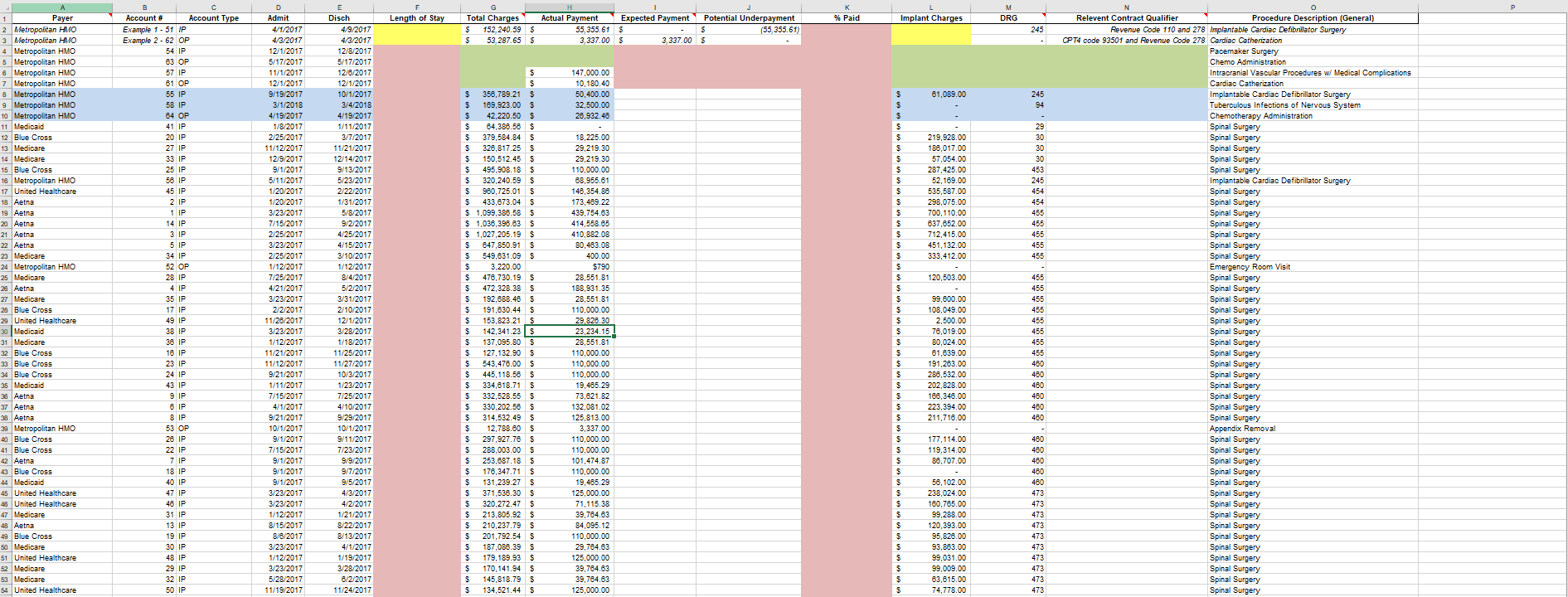
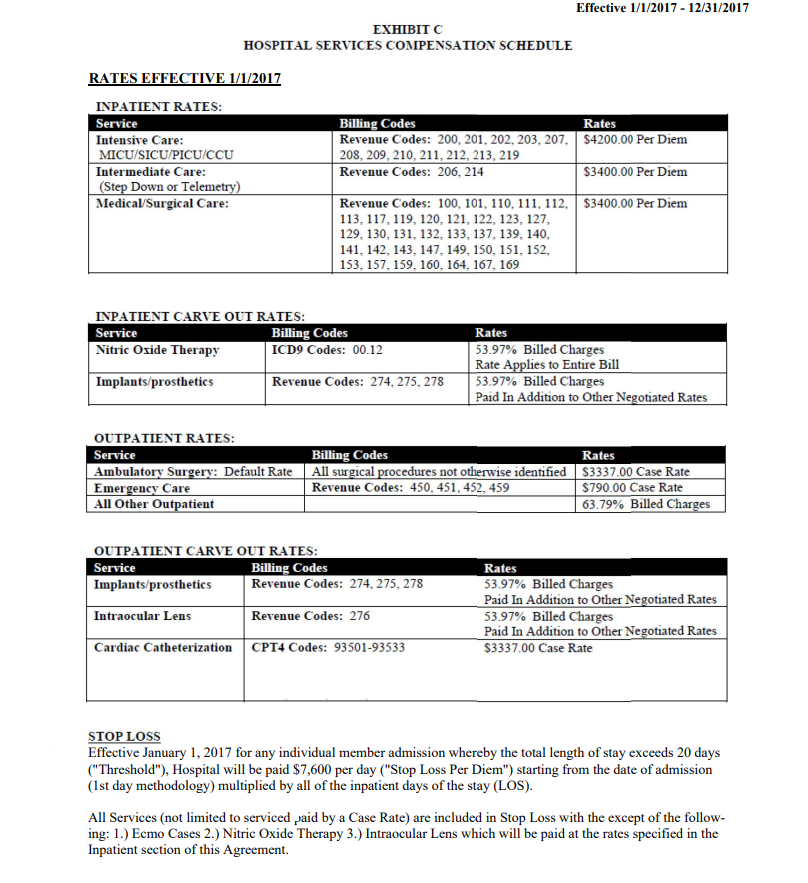
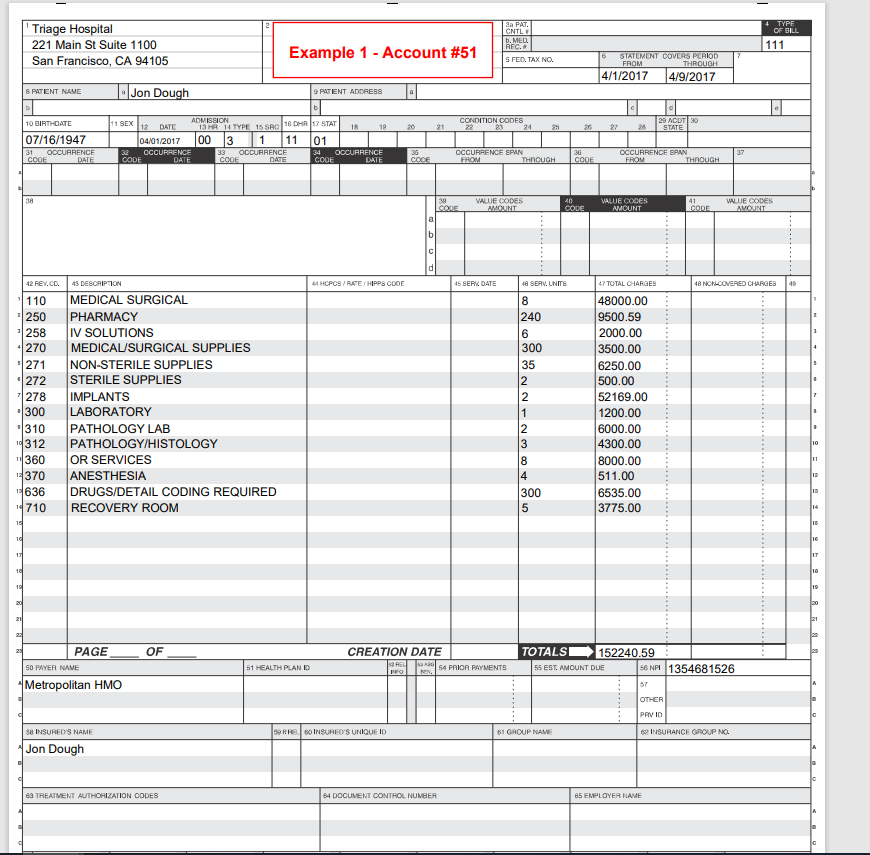
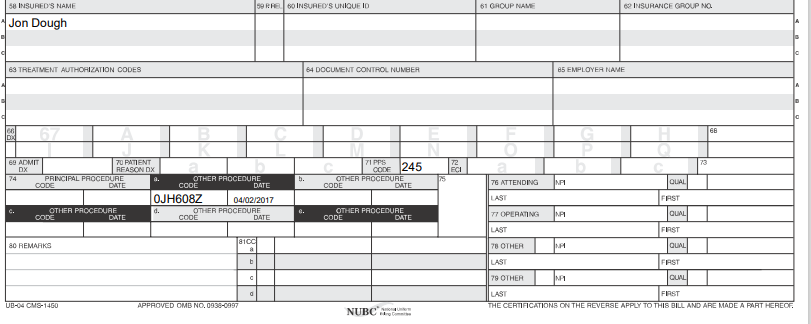
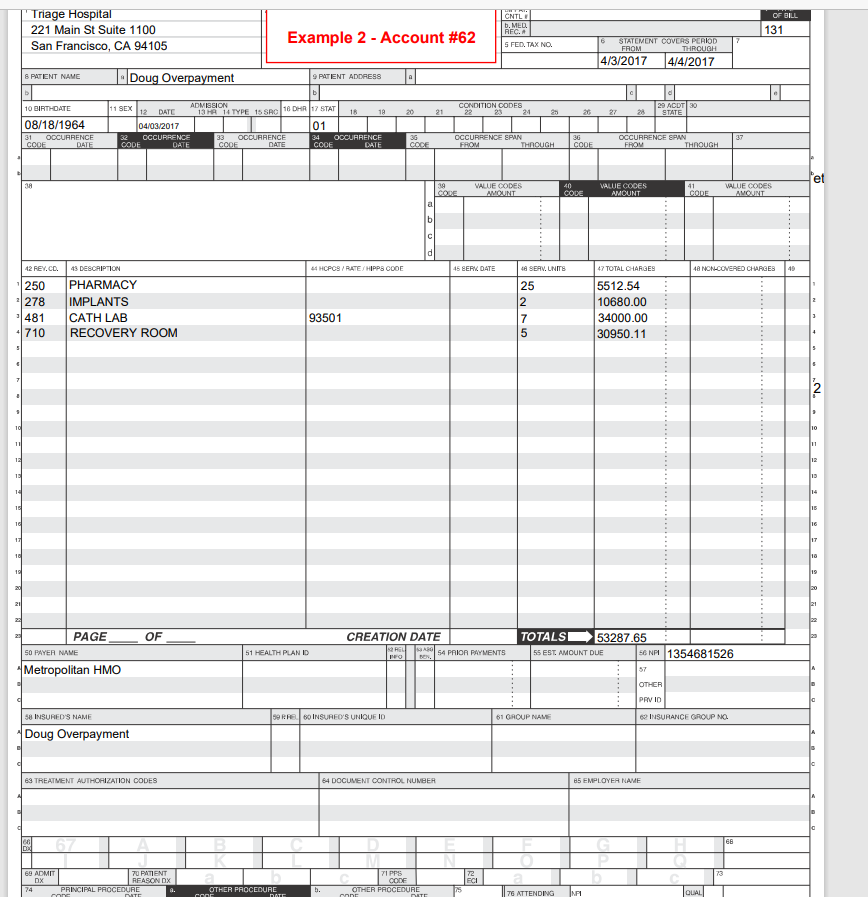
Data Analysis Case Study: Candidate Answers Example Question Please complete the cells higlighted in yellow on the 'Candidate Data' tab using the example UB-04s provided and data provided. This will provide guidance for Part 1 of the case study. 1) Completion Using the included EOBS, UB-04s, and Metropolitan HMO contract, please complete the cells higlighted in green on the 'Candidate Data' tab. The account numbers on the UB-04s correspond with the row in which the data should be filled in on the spreadsheet. 2) Computation Next, all cells highlighted in red require computation. Using the provided information and the information completed in Step 1, please fill in the cells highlighted in red. 3) Analysis Please use the information highlighted in blue and the Metropolitan HMO contract provided to answer the following questions. Using the data in each row, use the Metropolitan HMO contract provided to determine the methodology used by the payer to reimburse the claim? Please include the relevant contract provision and any other information to justify your answer Account #55: Account #58: Account #64: 4) Observations Step 4 is to draw observations from the entire data set given. Feel free to populated the 'Expected Payment' field as you see fit to help with your analysis. You may use the sentence format outlined below or write out your observations in bullets. Please provide exactly 5 of your best observations. You may adjust the size of any Observation cells as necessary. 4) Observations Step 4 is to draw observations from the entire data set given. Feel free to populated the 'Expected Payment' field as you see fit to help with your analysis. You may use the sentence format outlined below or write out your observations in bullets. Please provide exactly 5 of your best observations. You may adjust the size of any Observation cells as necessary. Example Observation: (do not update) The majority of the accounts where a Spinal Surgery occurred fall within the DRG range of 453-473. Those that fall outside of this range may have misreported the services provided to the applicable insurance company. Observation #1: Observation #2: Observation #3: Observation #4: Observation #5: Given your analysis from the steps above, please answer the scenario below. 5) Recommendations (Bonus) Cloudmed's client reached out with the provided data set ('Candidate Data"). Given your analysis of the data, which payer should the client prioritize in upcoming contract negotiations? Make sure to provide evidence of your recommendation. K % Paid M DRG Length of Stay Implant Charges Total Charges $ 152, 240.59 $ $ 53,287.65 $ Actual Payment Expected Payment Potential Underpayment 55,355.61 5 $ (55,355.61) 3,337.00 $ 3,337.00 $ 245 147,000.00 10,180.40 50,400.00 32,500.00 28,932.46 61,089.00 $ $ $ $ $ $ $ $ $ $ $ 219,928.00 188,017.00 57,054.00 287.425.00 52,169.00 535,587.00 298,075.00 700, 110.00 637,652.00 712,415.00 451,132.00 333,412.00 245 94 - 29 30 30 30 453 245 454 454 455 455 455 455 455 $ $ $ $ 120,503.00 1 Payer 2 Metropolitan HMO 3 Metropolitan HMO 4 Metropolitan HMO 5 Metropolitan HMO 6 Metropolitan HMO 7 Metropolitan HMO & Metropolitan HMO 9 Metropolitan HMO 10 Metropolitan HMO 11 Medicaid 12 Blue Cross 13 Medicare 14 Medicare 15 Blue Cross 16 Metropolitan HMO 17 United Healthcare 18 Aetna 19 Aetna 20 Aetna 21 Aetna 22 Aetna 23 Medicare 24 Metropolitan HMO 25 Medicare 26 Aetna 27 Medicare 28 Blue Cross 29 United Healthcare 30 Medicaid | 31 Medicare 32 Blue Cross 33 Blue Cross 34 Blue Cross 35 Medicaid 36 Aetna 37 Aetna 38 Aetna 39 Metropolitan HMO 40 Blue Cross 41 Blue Cross 42 Aetna 43 Blue Cross 44 Medicaid 45 United Healthcare 48 United Healthcare 47 Medicare 48 Aetna 49 Blue Cross 50 Medicare 51 United Healthcare 52 Medicare 53 Medicare 54 United Healthcare B Account # Account Type Example 1 - 51 IP Example 2 - 62 OP 54 IP 63 OF 57 IP 81 OF 55 IP 58 IP 84 OP 41 IP 20 IP 27 IP 33 IP 25 IP 56 IP 45 IP 2 IP 1 IP 14 IP 3 IP 5 IP 34 IP 52 OP 28 IP 4 IP 35 IP 17 IP 49 IP 38 IP 38 IP 16 IP 23 IP 24 IP 43 IP 9 IP 6 IP 8 IP 53 OP 28 IP 22 IP 7 IP 18 IP 40 IP 47 IP 46 IP 31 IP 13 IP 19 IP 30 IP 48 IP 29 IP 32 IP 50 IP D Admit 4/1/2017 4/3/2017 12/1/2017 5/17/2017 11/1/2017 12/1/2017 9/19/2017 3/1/2018 4/19/2017 1/8/2017 2/25/2017 11/12/2017 12/9/2017 9/1/2017 5/11/2017 1/20/2017 1/20/2017 3/23/2017 7/15/2017 2/25/2017 3/23/2017 2/25/2017 1/12/2017 7/25/2017 4/21/2017 3/23/2017 2/2/2017 11/26/2017 3/23/2017 1/12/2017 11/21/2017 11/12/2017 9/21/2017 1/11/2017 7/15/2017 4/1/2017 9/21/2017 10/1/2017 9/1/2017 7/15/2017 9/1/2017 9/1/2017 9/1/2017 3/23/2017 3/23/2017 1/12/2017 8/15/2017 8/6/2017 3/23/2017 1/12/2017 3/23/2017 5/28/2017 11/19/2017 Disch 4/9/2017 4/3/2017 12/8/2017 5/17/2017 12/6/2017 12/1/2017 10/1/2017 3/4/2018 4/19/2017 1/11/2017 3/7/2017 11/21/2017 12/14/2017 9/13/2017 5/23/2017 2/22/2017 1/31/2017 5/8/2017 9/2/2017 4/25/2017 4/15/2017 3/10/2017 1/12/2017 8/4/2017 5/2/2017 3/31/2017 2/10/2017 12/1/2017 3/28/2017 1/18/2017 11/25/2017 11/27/2017 10/3/2017 1/23/2017 7/25/2017 4/10/2017 9/29/2017 10/1/2017 9/11/2017 7/23/2017 9/9/2017 9/7/2017 9/5/2017 4/3/2017 4/2/2017 1/21/2017 8/22/2017 8/13/2017 4/1/2017 1/19/2017 3/28/2017 6/2/2017 11/24/2017 $ $ $ 358,789.21 $ $ 169,923.00 $ $ 42,220.50 $ $ 64,386.56 $ $ 379,584.84 5 $ $ 328,817.25 $ $ 150,512.45 $ $ 495,908.18 5 $ 320,240.59 $ $ 960,725.01 5 $ 433,673.04 5 $ $ 1,099,386.58 5 $ 1,038,396.63 $ $ 1,027,205.19 $ 647,850.91 $ $ 549,631.09 $ $ 3,220.00 $ $ 476,730.19 $ $ 472,328.38 $ $ 192,688.46 $ $ $ 191,630.44 $ $ 153,823.21 $ $ $ 142,341.235 $ 137.095.80 $ $ 127,132.90 $ $ 543,476.00 $ $ 445,118.56 $ $ 334,618.71 $ $ 332,528.55 $ $ 330,202.56 $ $ 314,532.49 $ $ 12,788.80 $ $ $ 297,927.76 $ $ $ 288,003.00 $ $ 253,687.18 $ $ 178,347.71 $ 131,239.27 $ $ 371,538.30 $ $ 320,272.47 5 $ 213,805.92 $ $ 210,237.79 $ $ $ 201,792.54 5 $ $ 187,088.39 $ $ 179,189.93 $ $ 170,141.94 $ $ 145,818.79 $ $ 134,521.44 $ 18,225.00 29,219.30 29,219.30 110,000.00 68,955.61 148,354.88 173,489.22 439,754.63 414,558.65 410.882.08 80,483.08 400.00 $790 $ 28,551.81 188,931.35 28,551.81 110,000.00 29.828.30 23,234.15 28,551.81 110,000.00 110,000.00 110,000.00 19,465.29 73.621.82 132.081.02 125,813.00 3,337.00 110,000.00 110,000.00 101,474.87 110,000.00 19,465.29 125,000.00 71,115,38 39,764.63 84,095.12 110,000.00 29,764.63 125,000.00 39,764.63 39,764.63 125,000.00 $ $ $ $ $ $ $ $ $ 99,800.00 108,049.00 2,500.00 78.019.00 80.024.00 61,639.00 191,283.00 288,532.00 202,828.00 168,346.00 223,394.00 211,716.00 455 455 455 455 455 455 455 455 480 480 460 480 480 480 Relevent Contract Qualifier Procedure Description (General) Revenue Code 110 and 278 Implantable Cardiac Defibrillator Surgery CPT4 code 93501 and Revenue Code 278 Cardiac Catherization Pacemaker Surgery Chemo Administration Intracranial Vascular Procedures w/ Medical Complications Cardiac Catherization Implantable Cardiac Defibrillator Surgery Tuberculous Infections of Nervous System Chemotherapy Administration Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Implantable Cardiac Defibrillator Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Emergency Room Visit Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Appendix Removal Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery 177,114.00 119,314.00 88,707.00 $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ 56,102.00 238,024.00 180,785.00 99,288.00 120,393.00 95,828.00 93,883.00 99,031.00 99,009.00 63,615.00 74,778.00 460 480 460 480 480 473 473 473 473 473 473 473 473 473 473 67,585.00 49,199.00 45,708.00 44,911.00 55 Medicaid 58 Aetna 57 Medicaid 58 Aetna 59 Aetna 60 United Healthcare 61 Blue Cross 62 Blue Cross 63 Medicaid 37 IP 12 IP 39 IP 10 IP 11 IP 44 IP 15 IF 21 IP 42 IP 1/13/2017 4/1/2017 1/12/2017 9/24/2017 3/12/2017 10/28/2017 4/1/2017 1/12/2017 1/12/2017 1/19/2017 4/5/2017 1/17/2017 9/28/2017 3/15/2017 11/20/2017 4/27/2017 3/25/2017 1/23/2017 $ 132,801.00 $ $ 128,337.34 $ $ 114,607.31 $ $ 105,133.42 $ $ 89,537.28 $ $ 755,593.54 5 $ 788,623.49 $ $ 1,232,088.46 5 $ 303,127.23 $ 28,314.38 51,334.94 28,314.38 42,053.37 35,814.90 147,982.24 110,000.00 110,000.00 48,257.22 $ $ $ $ $ $ $ $ $ 473 473 473 473 473 480 854 958 982 Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery 34,054.00 312,312.00 442,740.00 127,216.00 Effective 1/1/2017 - 12/31/2017 EXHIBIT C HOSPITAL SERVICES COMPENSATION SCHEDULE RATES EFFECTIVE 1/1/2017 INPATIENT RATES: Service Billing Codes Rates Intensive Care: Revenue Codes: 200, 201, 202, 203, 207, $4200.00 Per Diem MICU/SICU/PICU/CCU 208, 209, 210, 211, 212, 213, 219 Intermediate Care: Revenue Codes: 206, 214 $3400.00 Per Diem (Step Down or Telemetry) Medical/Surgical Care: Revenue Codes: 100, 101, 110, 111, 112, $3400.00 Per Diem 113, 117, 119, 120, 121, 122, 123, 127, 129, 130, 131, 132, 133, 137, 139, 140, 141, 142, 143, 147, 149, 150, 151, 152, 153, 157, 159, 160, 164, 167, 169 INPATIENT CARVE OUT RATES: Service Billing Codes Nitric Oxide Therapy ICD9 Codes: 00.12 Implants/prosthetics Revenue Codes: 274, 275, 278 Rates 53.97% Billed Charges Rate Applies to Entire Bill 53.97% Billed Charges Paid In Addition to Other Negotiated Rates OUTPATIENT RATES: Service Ambulatory Surgery: Default Rate Emergency Care All Other Outpatient Billing Codes Rates All surgical procedures not otherwise identified $3337.00 Case Rate Revenue Codes: 450, 451, 452, 459 $790.00 Case Rate 63.79% Billed Charges OUTPATIENT CARVE OUT RATES: Service Billing Codes Implants/prosthetics Revenue Codes: 274, 275, 278 Intraocular Lens Revenue Codes: 276 Rates 53.97% Billed Charges Paid In Addition to Other Negotiated Rates 53.97% Billed Charges Paid In Addition to Other Negotiated Rates $3337.00 Case Rate Cardiac Catheterization CPT4 Codes: 93501-93533 STOP LOSS Effective January 1, 2017 for any individual member admission whereby the total length of stay exceeds 20 days ("Threshold"), Hospital will be paid $7,600 per day ("Stop Loss Per Diem") starting from the date of admission (1st day methodology) multiplied by all of the inpatient days of the stay (LOS). All Services (not limited to serviced aid by a Case Rate) are included in Stop Loss with the except of the follow- ing: 1.) Ecmo Cases 2.) Nitric Oxide Therapy 3.) Intraocular Lens which will be paid at the rates specified in the Inpatient section of Agreement. Triage Hospital 221 Main St Suite 1100 San Francisco, CA 94105 3a PAT. CNTL RFC. 5. MED. 4 TYPE OF BILL 111 Example 1 - Account #51 S FED. TAX NO. 6 STATEMENT COVERS PERIOD FROM THROUGH 4/1/2017 4/9/2017 S PATIENT NAME 1. Jon Dough 9 PATIENT ADDRESS 10 BIRTHDATE 20 21 CONDITION CODES 22 23 24 29 ACDT30 STATE 27 28 11 SEX ADMISSION 12 DATE 13 H 14 TYPE 15 SRC 16DHR17 STAT 18 18 04/01/2017 00 3 1 11 OCCURRENCE 33 OCCURRENCE 34 CODE OCCURRENCE CODE DATE CODE DATE 01 07/16/1947 31 OCCURRENCE CODE DATE 37 36 CODE OCCURRENCE SPAN FROM THROUGH 36 CODE OCCURRENCE SPAN FROM THROUGH 38 39 40 41 VALUE CODES AMOUNT VALUE CODES AMOUNT VALUE CODES AMOUNT al b d 42 REY.CL. 43 DESCRIPTION 64 HCPCS / RATE/HIPPS COOE 45 BERK DATE 47 TOTAL CHARGES 48 NON COVERED CHARGES 49 110 1250 1258 + 270 271 272 1278 300 *310 10312 11360 - 370 1636 14710 MEDICAL SURGICAL PHARMACY IV SOLUTIONS MEDICAL SURGICAL SUPPLIES NON-STERILE SUPPLIES STERILE SUPPLIES IMPLANTS LABORATORY PATHOLOGY LAB PATHOLOGY/HISTOLOGY OR SERVICES ANESTHESIA DRUGS/DETAIL CODING REQUIRED RECOVERY ROOM 4 SERV. UNITS 8 240 6 300 35 2 2 1 48000.00 9500.59 2000.00 3500.00 6250.00 500.00 52169.00 1200.00 6000.00 4300.00 8000.00 511.00 6535.00 3775.00 10 11 12 8 4 300 5 + 9 13 14 16 16 10 16 17 IT 16 10 16 19 20 21 21 OF CREATION DATE PAGE 50 PAYER NAME Metropolitan HMO TOTALS 152240.59 55 EST AMOUNT DUE 56 NP 1354681526 51 HEALTH PLAN ID RU O ARO BEN, 54 PAIOR PAYMENTS 57 OTHER PRVID SORREO INSURE'S UNIQUE ID 61 GROUP NAME 62 INSURANCE GROUP NO. 58 INSURED'S NAME Jon Dough 68 TREATMENT AUTHORIZATION CODES 64 DOCUMENT CONTROL NUMBER 85 EMPLOYER NAME 59RFEINSURES UNIQUE ID 61 GROUP NAME 62 INSURANCE GROUP NO 58 INSURED'S NAME Jon Dough 68 TREATMENT AUTHORIZATION CODES 64 DOCUMENT CONTROL NUMBER 85 EMPLOYER NAME CA DA 68 87 C 73 CODE 245 72 ECI 7 PPS OTHER PROCEDURE CODE DATE b. 76 ATTENDING 69 ADMIT 70 PATIENT DX REASON DX 74 PRINCIPAL PROCEDURE A. OTHER PROCEDURE CODE DATE CODE DATE OJH608Z 04/02/2017 C. OTHER PROCEDURE d. OTHER PROCEDURE CODE DATE CODE DATE NFI QUAL FAST LASI CODE OTHER PROCEDURE DATE 77 OPERATING NAI QUAL LAST FIRST 80 REMARKS 8100 78 OTHER QUAL b LAST FEST G 79 OTHER NA CUAL LAST FIRST THE CERTIFICATIONS ON THE REVERSE APPLY TO THIS BILL AND ARE MADE A PART HEREOF. UB-04 CMS-1460 APPROVED OMB NO. 0938-0997 NUBC Triage Hospital 221 Main St Suite 1100 San Francisco, CA 94105 CNTL b. MED REC. S FED. TAX NO. OF BILL 131 Example 2 - Account #62 6 STATEMENT COVERS PERIOD FROM THROUGH 4/3/2017 4/4/2017 S PATIENT NAME Doug Overpayment 9 PATENT ADDRESS CONDITION CODES 22 24 29 ACDT 30 21 27 STATE 10 BIRTHDATE 08/18/1964 31 OCCURRENCE COOF DATE 11 SEX ADMISSION 12 DATE 13 HA 14 TYPE 15 SRO 16 DHR17 STAT 18 18 04/03/2017 01 32 OCCURRENCE 33 OCCURRENCE 34 CODE OCCURRENCE DATE DATE CODE DATE 36 37 36 CORE OCCURRENCE SPAN FROM THROUGH CODE OCCURRENCE SPAN FROM THROUGH et 3A 19 41 VALUE CODES AMOUNT 40 CODE VALUE CODES AMOUNT CODE VALUE CODES AMOUNT a b d 4 HCPCS / RATE/HIPPS CODE 45 BERK DATE 48 NON COVERED CHARGES 49 12 REY.CO. 45 DESCRIPTION 250 PHARMACY 1278 IMPLANTS 1481 CATH LAB +1 710 RECOVERY ROOM 4 SERV. UNITS 25 2 7 5 47 TOTAL CHARGES 5512.54 10680.00 34000.00 30950.11 93501 3 2 'N 10 111 11 1E 12 15 14 14 TE 15 10 16 151 16 10 15 19 20 20 21 21 OF CREATION DATE PAGE 50 PAYER NAME TOTALS 53287.65 55 EST AMOUNT DUE 56 NPI 1354681526 ROL SARO 51 HEALTH PLAN ID 54 PAIOR PAYMENTS Metropolitan HMO 57 OTHER PRVID 58 INSURED'S NAME 59RRE. BINSURED'S UNIQUE ID 61 GROUP NAM 62 INSURANCE GROUP NO. Doug Overpayment 68 TREATMENT AUTHORIZATION CODES 64 DOCUMENT CONTROL NUMBER 85 EMPLOYER NAME 68 100 IDB TIPPS 69 ADMIT DX 74 70 PATIENT REASON DX PRINCIPAL PROCEDURE Tr CODE 72 ECI OTHER PROCEDURE oor DATE b. OTHER PROCEDURE CODE 76 ATTENDING NAI QUAL Triage Hospital 221 Main St Suite 1100 San Francisco, CA 94105 3a PAT, CNTL b. MLD AFC. 4 TYPE OF BILL 111 Account #54 7 S FED. TAX NO. 6 STATEMENT COVERS PERIOD FROM THROUGH 12/1/2017 12/8/2017 S PATIENT NAME Tom Montana 9 PATIENT ADDRESS 11 SEX 12 21 CONDITION CODES 22 23 24 27 28 29 ACDT 30 STATE 10 BIRTHDATE 01/20/1950 31 OCCURRENCE COOF DATE ADMISSION DATE 13 R 14 TYPE 15 SRO 18 DHR17 STAT 18 18 12/01/2017 003 1 11 01 32 OCCURRENCE 33 OCCURRENCE 34 CODE OCCURRENCE DATE DATE CODE DATE 37 CODE 36 COCE OCCURRENCE SPAN FROM THROUGH 36 COOF OCCURRENCE SPWN FROM THROUGH 3 19 CORE al VALUE CODES AMOUNT 40 CODE VALUE CODES AMOUNT 41 CORE VALUE CODES AMOUNT b c d 42 REY.CO. 64 HCPCS / RATE/HIPPS COOE 45 BERN DATE 18 SERV, UNITS 48 NON-COVERED CHARGES 49 110 250 -258 4270 271 272 7 278 .300 310 10312 1360 15370 1636 14710 43 DESCRIPTION MEDICAL SURGICAL PHARMACY IV SOLUTIONS MEDICAL SURGICAL SUPPLIES NON-STERILE SUPPLIES STERILE SUPPLIES IMPLANTS LABORATORY PATHOLOGY LAB PATHOLOGY/HISTOLOGY OR SERVICES ANESTHESIA DRUGS/DETAIL CODING REQUIRED RECOVERY ROOM 7 240 6 250 35 2 2 1 4 3 8 4 300 5 47 TOTAL CHARGES 42000.00 5500.59 1000.00 4411.00 6250.00 500.00 42258.00 1200.00 2000.00 4300.00 4000.00 511.00 5535.00 3775.00 111 12 14 TE lis 1 lig 171 16 lig 15 19 20 211 21 OF PAGE 50 PAYER NAME Metropolitan HMO CREATION DATE ABO 54 PAIOR PAYMENTS TOTALS 123240.59 55 EST. AMOUNT DUE 56 NP 1354681526 51 HEALTH PLAN ID 57 OTHER PRVID INSURANCE GROUP NO. SORREO INSURED'S UNIQUE ID 61 GROUP NAME 58 INSURED'S NAME Tom Montana 63 TREATMENT AUTHORIZATION CODES 64 DOCUMENT CONTROL NUMBER 85 EMPLOYER NAME CA DA 68 TIPPS 69 ADMIT DX 74 73 70 PATIENT REASON DX PRINCIPAL PROCEDURE 72 ECI CODE 243 OTHER PROCEDURE b. OTHER PROCEDURE 'Triage Hospital 221 Main St Suite 1100 San Francisco, CA 94105 3a PAT. CNTL b.MED. RFC. 4 TYPE OF BILL 131 Account #63 6 S FED. TAX NO. STATEMENT COVERS PERIOD FROM THROUGH 5/17/2017 5/17/2017 S PATENT NAME Vivian Variance 9 PATENT ADDRESS CONDITION CODES 22 22 21 25 27 29 ACDT 30 STATE 28 10 BIRTHDATE 03/22/1976 31 OCCURRENCE COOF DATE 11 SEX ADMISSION 12 DATE 13 PR 14 TYPE 15 SRC 16DHR 17 STAT 18 10 05/17/2017 01 32 OCCURRENCE 33 OCCURRENCE 34 CODE OCCURRENCE DATE COOF DATE CODE DATE 37 36 COCE OCCURRENCE SPAN FROM THROUGH 36 COOF OCCURRENCE SPAN FROM THROUGH et 38 19 VALUJE CODES AMOUNT 40 COLE VALUE CODES AMOUNT 41 CORE VALLIE CODES AMOUNT a b d 42 REV.CD 44 HCPCS / RATE/HIPPS COOL 45 BERK DATE 4a NONCOVERED CHARGES 49 250 1335 636 4710 43 DESCRIPTION PHARMACY CHEMOTHERAPY/IV DRUGS/DETAIL CODE RECOVERY ROOM 48 SERV. UNITS 3 8 200 1 47 TOTAL CHARGES 200.00 3500.00 57840.00 1000.00 J9299 5 2 10 11 111 15 12 1E 13 14 14 TE 15 10 16 17 10 10 15 19 20 20 21 21 OF PAGE 50 PAYER NAME Metropolitan HMO CREATION DATE REL PO , 54 PAIOR PAYMENTS 51 HEALTH PLAN ID TOTALSI 62540.00 55 EST AMOUNT DUE 56 NP 1354681526 57 OTHER PRVID SORRE COINSURED'S UNIQUE ID 61 GROUP NAME 6 INSURANCE GROUP NO. 58 INSURED'S NAME Vivian Variance 69 TREATMENT AUTHORIZATION CODES 64 DOCUMENT CONTROL NUMBER 85 EMPLOYER NAME A D 68 06 DO A 69 ADMIT 772 70 PATIENT BEACONY 73 71 PPE cond suite Account #57 AFC. S FED, TAX NO 6 San Francisco, CA 94105 STATEMENT COVERS PERIOD FROM THROUGH 11/1/2017 12/6/2017 & PATIENT NAME - Betsy Ross 9 PATENT ADDRESS 20 21 CONDITION CODES 22 23 24 27 28 29 ACDT 30 STATE 10 BIRTHDATE 05/25/1953 31 OCCURRENCE COOF DATE 11 SEX ADMISSION 12 DATE 13 H 14 TYPE IS SRO 10 DHR 1 STAT 18 18 11/01/2017 00 3 1 11 01 32 OCCURRENCE 33 OCCURRENCE 34 OCCURRENCE CODE DATE COOF DATE CODE DATE 36 37 OCCURRENCE SPAN FROM THROUGH 36 COOF OCCURRENCE SPAN FROM THROUGH et 3A 39 VALUE CODES AMOUNT 40 CODE VALUE CODES AMOUNT 41 CODE VALUE CODES AMOUNT a b d 43 DESCRIPTION 44 HCPCS / RATE / HIPPS COOE 45 BERK DATE 48 NONCOVERED CHARGES 40 12 REY.CO. 200 INTENSIVE CARE *250 PHARMACY 258 IV SOLUTIONS + 270 MEDICAL SURGICAL SUPPLIES 271 NON-STERILE SUPPLIES 272 STERILE SUPPLIES 278 IMPLANTS 300 LABORATORY 310 PATHOLOGY LAB 10312 PATHOLOGY/HISTOLOGY 11360 OR SERVICES 15370 ANESTHESIA 636 DRUGS/DETAIL CODING REQUIRED 14710 RECOVERY ROOM 15 48 SERV. UNITS 35 520 9 321 35 2 2 1 4 15 8 30 3250 5 47 TOTAL CHARGES 332500.00 16500.00 10000.00 4411.00 9250.00 3500.00 8600.00 5787.54 7000.00 53000.00 15000.00 12000.00 247466.00 3775.00 10 11 12 15 14 15 id 16 15 10 10 15 19 20 21 OF PAGE 50 PAYER NAME Metropolitan HMO CREATION DATE 54 PRIOR PAYMENTS 51 HEALTH PLAN D TOTALSI 728789.54 55 EST AMOUNT DUE 56 NP 1354681526 57 OTHER PRVID 58 INSURED'S NAME SORREO INSURED'S UNIQUE ID 61 GROUP NAME 2 INSURANCE GROUP NO. Betsy Ross 68 TREATMENT AUTHORIZATION CODES 64 DOCUMENT CONTROL NUMBER 85 EMPLOYER NAME 100 DO 68 TIPP 73 CODE 20 ECI IS 69 ADMIT 70 PATIENT DX REASON DX 74 PRINCIPAL PROCEDURE OTHER PROCEDURE CODE DATE CODE DATE B313YZZ 11/01/2017 03VG3DZ 11/01/2017 76 ATTENDING NAI QUAL b. OTHER PROCEDURE CODE DATE 02HV33Z 11/20/2017 LAST FIRST Triage Hospital 221 Main St Suite 1100 San Francisco, CA 94105 2a PAT. CNTL b. MED REG. S FED. TAX NO. 4 TYPE OF BILL 131 Account #61 7 6 STATEMENT COVERS PERIOD FROM THROUGH 12/1/2017 12/2/2017 S PATIENT NAME Frank Underpayment 9 PATENT ADDRESS 21 CONDITION CODES 22 23 24 27 28 29 ACDT 30 STATE 10 BIRTHDATE 09/14/1955 31 OCCURRENCE COOE DATE 11 SEX ADMISSION 12 DATE 131 14 TYPE 15 SRC 18 DHR 17 STAT 18 18 12/01/2017 101 32 OCCURRENCE 33 OCCURRENCE 34 OCCURRENCE CODE 14 CODEDATE CODE_DATE 37 COCE OCCURRENCE EPAN FROM THROUGH 36 COOF OCCURRENCE EPWN FROM THROUGH et 38 39 CODE a VALLE CODES AMOUNT 40 COLE VALUE CODES BAUMIT 41 CORE VALLE CODES AMOUNT b d 12 REX.CO. 4 HCPCS / RATE/HIPPS COOL 45 BERK DATE 4 SERV. UNITS 48 NONCOVERED CHARGES 49 27 250 278 481 + 710 45 DESCRIPTION PHARMACY IMPLANTS CATH LAB RECOVERY ROOM 47 TOTAL CHARGES 4512.54 12680.00 32500.00 2986.00 93525 2 10 10 11 1E 12 JE 13 14 14 11 15 1 16 17 IT 13 10 15 19 20 20 21 21 OF PAGE 50 PAYER NAME Metropolitan HMO CREATION DATE AR O sex 54 PRIOR PAYMENTS NARO TOTALSI 52678.54 55 EST. AMOUNT DUE 56 NPI 1354681526 51 HEALTH PLAN ID 57 OTHER PRVID 58 INSURED'S NAME SORREO INSURED'S UNIQUE ID 61 GROUP NAME 62 INSURANCE GROUP NO Frank Underpayment 63 TREATMENT AUTHORIZATION CODES 64 DOCUMENT CONTROL NUMBER 85 EMPLOYER NAME 100 ID 68 69 ADMIT 70 PATIENT 7IPPS 72 TE Explanation of Benefits - Account #54 Patient Name Tom Montana Account 54 ID A11332211 Plan Dates of Service Metropolitan HMO 12/1/2017 - 12/8/2017 Excluded Disallowed Allowed Amount 23,800.00 Patient Responsibility 500.00 Benefit Paid 23,200.00 Expenses 110 42,000.00 278 42,258.00 Other 38,982.59 Total 123,240.59 42,258.00 38,982.59 38,982.59 23,800.00 42,258.00 500.00 23,300.00 Explanation of Benefits - Account #63 Patient Name Vivian Variance Account 63 ID A99955599 Plan Dates of Service Metropolitan HMO 5/17/2017 - 5/17/2017 Disallowed Expenses Other 62,540.00 Total 62,540.00 Excluded 62,540.00 62,540.00 Allowed Amount 39,894.27 39,894.27 Patient Responsibility Benefit Paid 1,000.00 38,894.27 1,000.00 38,894.27 Data Analysis Case Study: Candidate Answers Example Question Please complete the cells higlighted in yellow on the 'Candidate Data' tab using the example UB-04s provided and data provided. This will provide guidance for Part 1 of the case study. 1) Completion Using the included EOBS, UB-04s, and Metropolitan HMO contract, please complete the cells higlighted in green on the 'Candidate Data' tab. The account numbers on the UB-04s correspond with the row in which the data should be filled in on the spreadsheet. 2) Computation Next, all cells highlighted in red require computation. Using the provided information and the information completed in Step 1, please fill in the cells highlighted in red. 3) Analysis Please use the information highlighted in blue and the Metropolitan HMO contract provided to answer the following questions. Using the data in each row, use the Metropolitan HMO contract provided to determine the methodology used by the payer to reimburse the claim? Please include the relevant contract provision and any other information to justify your answer Account #55: Account #58: Account #64: 4) Observations Step 4 is to draw observations from the entire data set given. Feel free to populated the 'Expected Payment' field as you see fit to help with your analysis. You may use the sentence format outlined below or write out your observations in bullets. Please provide exactly 5 of your best observations. You may adjust the size of any Observation cells as necessary. 4) Observations Step 4 is to draw observations from the entire data set given. Feel free to populated the 'Expected Payment' field as you see fit to help with your analysis. You may use the sentence format outlined below or write out your observations in bullets. Please provide exactly 5 of your best observations. You may adjust the size of any Observation cells as necessary. Example Observation: (do not update) The majority of the accounts where a Spinal Surgery occurred fall within the DRG range of 453-473. Those that fall outside of this range may have misreported the services provided to the applicable insurance company. Observation #1: Observation #2: Observation #3: Observation #4: Observation #5: Given your analysis from the steps above, please answer the scenario below. 5) Recommendations (Bonus) Cloudmed's client reached out with the provided data set ('Candidate Data"). Given your analysis of the data, which payer should the client prioritize in upcoming contract negotiations? Make sure to provide evidence of your recommendation. K % Paid M DRG Length of Stay Implant Charges Total Charges $ 152, 240.59 $ $ 53,287.65 $ Actual Payment Expected Payment Potential Underpayment 55,355.61 5 $ (55,355.61) 3,337.00 $ 3,337.00 $ 245 147,000.00 10,180.40 50,400.00 32,500.00 28,932.46 61,089.00 $ $ $ $ $ $ $ $ $ $ $ 219,928.00 188,017.00 57,054.00 287.425.00 52,169.00 535,587.00 298,075.00 700, 110.00 637,652.00 712,415.00 451,132.00 333,412.00 245 94 - 29 30 30 30 453 245 454 454 455 455 455 455 455 $ $ $ $ 120,503.00 1 Payer 2 Metropolitan HMO 3 Metropolitan HMO 4 Metropolitan HMO 5 Metropolitan HMO 6 Metropolitan HMO 7 Metropolitan HMO & Metropolitan HMO 9 Metropolitan HMO 10 Metropolitan HMO 11 Medicaid 12 Blue Cross 13 Medicare 14 Medicare 15 Blue Cross 16 Metropolitan HMO 17 United Healthcare 18 Aetna 19 Aetna 20 Aetna 21 Aetna 22 Aetna 23 Medicare 24 Metropolitan HMO 25 Medicare 26 Aetna 27 Medicare 28 Blue Cross 29 United Healthcare 30 Medicaid | 31 Medicare 32 Blue Cross 33 Blue Cross 34 Blue Cross 35 Medicaid 36 Aetna 37 Aetna 38 Aetna 39 Metropolitan HMO 40 Blue Cross 41 Blue Cross 42 Aetna 43 Blue Cross 44 Medicaid 45 United Healthcare 48 United Healthcare 47 Medicare 48 Aetna 49 Blue Cross 50 Medicare 51 United Healthcare 52 Medicare 53 Medicare 54 United Healthcare B Account # Account Type Example 1 - 51 IP Example 2 - 62 OP 54 IP 63 OF 57 IP 81 OF 55 IP 58 IP 84 OP 41 IP 20 IP 27 IP 33 IP 25 IP 56 IP 45 IP 2 IP 1 IP 14 IP 3 IP 5 IP 34 IP 52 OP 28 IP 4 IP 35 IP 17 IP 49 IP 38 IP 38 IP 16 IP 23 IP 24 IP 43 IP 9 IP 6 IP 8 IP 53 OP 28 IP 22 IP 7 IP 18 IP 40 IP 47 IP 46 IP 31 IP 13 IP 19 IP 30 IP 48 IP 29 IP 32 IP 50 IP D Admit 4/1/2017 4/3/2017 12/1/2017 5/17/2017 11/1/2017 12/1/2017 9/19/2017 3/1/2018 4/19/2017 1/8/2017 2/25/2017 11/12/2017 12/9/2017 9/1/2017 5/11/2017 1/20/2017 1/20/2017 3/23/2017 7/15/2017 2/25/2017 3/23/2017 2/25/2017 1/12/2017 7/25/2017 4/21/2017 3/23/2017 2/2/2017 11/26/2017 3/23/2017 1/12/2017 11/21/2017 11/12/2017 9/21/2017 1/11/2017 7/15/2017 4/1/2017 9/21/2017 10/1/2017 9/1/2017 7/15/2017 9/1/2017 9/1/2017 9/1/2017 3/23/2017 3/23/2017 1/12/2017 8/15/2017 8/6/2017 3/23/2017 1/12/2017 3/23/2017 5/28/2017 11/19/2017 Disch 4/9/2017 4/3/2017 12/8/2017 5/17/2017 12/6/2017 12/1/2017 10/1/2017 3/4/2018 4/19/2017 1/11/2017 3/7/2017 11/21/2017 12/14/2017 9/13/2017 5/23/2017 2/22/2017 1/31/2017 5/8/2017 9/2/2017 4/25/2017 4/15/2017 3/10/2017 1/12/2017 8/4/2017 5/2/2017 3/31/2017 2/10/2017 12/1/2017 3/28/2017 1/18/2017 11/25/2017 11/27/2017 10/3/2017 1/23/2017 7/25/2017 4/10/2017 9/29/2017 10/1/2017 9/11/2017 7/23/2017 9/9/2017 9/7/2017 9/5/2017 4/3/2017 4/2/2017 1/21/2017 8/22/2017 8/13/2017 4/1/2017 1/19/2017 3/28/2017 6/2/2017 11/24/2017 $ $ $ 358,789.21 $ $ 169,923.00 $ $ 42,220.50 $ $ 64,386.56 $ $ 379,584.84 5 $ $ 328,817.25 $ $ 150,512.45 $ $ 495,908.18 5 $ 320,240.59 $ $ 960,725.01 5 $ 433,673.04 5 $ $ 1,099,386.58 5 $ 1,038,396.63 $ $ 1,027,205.19 $ 647,850.91 $ $ 549,631.09 $ $ 3,220.00 $ $ 476,730.19 $ $ 472,328.38 $ $ 192,688.46 $ $ $ 191,630.44 $ $ 153,823.21 $ $ $ 142,341.235 $ 137.095.80 $ $ 127,132.90 $ $ 543,476.00 $ $ 445,118.56 $ $ 334,618.71 $ $ 332,528.55 $ $ 330,202.56 $ $ 314,532.49 $ $ 12,788.80 $ $ $ 297,927.76 $ $ $ 288,003.00 $ $ 253,687.18 $ $ 178,347.71 $ 131,239.27 $ $ 371,538.30 $ $ 320,272.47 5 $ 213,805.92 $ $ 210,237.79 $ $ $ 201,792.54 5 $ $ 187,088.39 $ $ 179,189.93 $ $ 170,141.94 $ $ 145,818.79 $ $ 134,521.44 $ 18,225.00 29,219.30 29,219.30 110,000.00 68,955.61 148,354.88 173,489.22 439,754.63 414,558.65 410.882.08 80,483.08 400.00 $790 $ 28,551.81 188,931.35 28,551.81 110,000.00 29.828.30 23,234.15 28,551.81 110,000.00 110,000.00 110,000.00 19,465.29 73.621.82 132.081.02 125,813.00 3,337.00 110,000.00 110,000.00 101,474.87 110,000.00 19,465.29 125,000.00 71,115,38 39,764.63 84,095.12 110,000.00 29,764.63 125,000.00 39,764.63 39,764.63 125,000.00 $ $ $ $ $ $ $ $ $ 99,800.00 108,049.00 2,500.00 78.019.00 80.024.00 61,639.00 191,283.00 288,532.00 202,828.00 168,346.00 223,394.00 211,716.00 455 455 455 455 455 455 455 455 480 480 460 480 480 480 Relevent Contract Qualifier Procedure Description (General) Revenue Code 110 and 278 Implantable Cardiac Defibrillator Surgery CPT4 code 93501 and Revenue Code 278 Cardiac Catherization Pacemaker Surgery Chemo Administration Intracranial Vascular Procedures w/ Medical Complications Cardiac Catherization Implantable Cardiac Defibrillator Surgery Tuberculous Infections of Nervous System Chemotherapy Administration Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Implantable Cardiac Defibrillator Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Emergency Room Visit Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Appendix Removal Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery 177,114.00 119,314.00 88,707.00 $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ 56,102.00 238,024.00 180,785.00 99,288.00 120,393.00 95,828.00 93,883.00 99,031.00 99,009.00 63,615.00 74,778.00 460 480 460 480 480 473 473 473 473 473 473 473 473 473 473 67,585.00 49,199.00 45,708.00 44,911.00 55 Medicaid 58 Aetna 57 Medicaid 58 Aetna 59 Aetna 60 United Healthcare 61 Blue Cross 62 Blue Cross 63 Medicaid 37 IP 12 IP 39 IP 10 IP 11 IP 44 IP 15 IF 21 IP 42 IP 1/13/2017 4/1/2017 1/12/2017 9/24/2017 3/12/2017 10/28/2017 4/1/2017 1/12/2017 1/12/2017 1/19/2017 4/5/2017 1/17/2017 9/28/2017 3/15/2017 11/20/2017 4/27/2017 3/25/2017 1/23/2017 $ 132,801.00 $ $ 128,337.34 $ $ 114,607.31 $ $ 105,133.42 $ $ 89,537.28 $ $ 755,593.54 5 $ 788,623.49 $ $ 1,232,088.46 5 $ 303,127.23 $ 28,314.38 51,334.94 28,314.38 42,053.37 35,814.90 147,982.24 110,000.00 110,000.00 48,257.22 $ $ $ $ $ $ $ $ $ 473 473 473 473 473 480 854 958 982 Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery Spinal Surgery 34,054.00 312,312.00 442,740.00 127,216.00 Effective 1/1/2017 - 12/31/2017 EXHIBIT C HOSPITAL SERVICES COMPENSATION SCHEDULE RATES EFFECTIVE 1/1/2017 INPATIENT RATES: Service Billing Codes Rates Intensive Care: Revenue Codes: 200, 201, 202, 203, 207, $4200.00 Per Diem MICU/SICU/PICU/CCU 208, 209, 210, 211, 212, 213, 219 Intermediate Care: Revenue Codes: 206, 214 $3400.00 Per Diem (Step Down or Telemetry) Medical/Surgical Care: Revenue Codes: 100, 101, 110, 111, 112, $3400.00 Per Diem 113, 117, 119, 120, 121, 122, 123, 127, 129, 130, 131, 132, 133, 137, 139, 140, 141, 142, 143, 147, 149, 150, 151, 152, 153, 157, 159, 160, 164, 167, 169 INPATIENT CARVE OUT RATES: Service Billing Codes Nitric Oxide Therapy ICD9 Codes: 00.12 Implants/prosthetics Revenue Codes: 274, 275, 278 Rates 53.97% Billed Charges Rate Applies to Entire Bill 53.97% Billed Charges Paid In Addition to Other Negotiated Rates OUTPATIENT RATES: Service Ambulatory Surgery: Default Rate Emergency Care All Other Outpatient Billing Codes Rates All surgical procedures not otherwise identified $3337.00 Case Rate Revenue Codes: 450, 451, 452, 459 $790.00 Case Rate 63.79% Billed Charges OUTPATIENT CARVE OUT RATES: Service Billing Codes Implants/prosthetics Revenue Codes: 274, 275, 278 Intraocular Lens Revenue Codes: 276 Rates 53.97% Billed Charges Paid In Addition to Other Negotiated Rates 53.97% Billed Charges Paid In Addition to Other Negotiated Rates $3337.00 Case Rate Cardiac Catheterization CPT4 Codes: 93501-93533 STOP LOSS Effective January 1, 2017 for any individual member admission whereby the total length of stay exceeds 20 days ("Threshold"), Hospital will be paid $7,600 per day ("Stop Loss Per Diem") starting from the date of admission (1st day methodology) multiplied by all of the inpatient days of the stay (LOS). All Services (not limited to serviced aid by a Case Rate) are included in Stop Loss with the except of the follow- ing: 1.) Ecmo Cases 2.) Nitric Oxide Therapy 3.) Intraocular Lens which will be paid at the rates specified in the Inpatient section of Agreement. Triage Hospital 221 Main St Suite 1100 San Francisco, CA 94105 3a PAT. CNTL RFC. 5. MED. 4 TYPE OF BILL 111 Example 1 - Account #51 S FED. TAX NO. 6 STATEMENT COVERS PERIOD FROM THROUGH 4/1/2017 4/9/2017 S PATIENT NAME 1. Jon Dough 9 PATIENT ADDRESS 10 BIRTHDATE 20 21 CONDITION CODES 22 23 24 29 ACDT30 STATE 27 28 11 SEX ADMISSION 12 DATE 13 H 14 TYPE 15 SRC 16DHR17 STAT 18 18 04/01/2017 00 3 1 11 OCCURRENCE 33 OCCURRENCE 34 CODE OCCURRENCE CODE DATE CODE DATE 01 07/16/1947 31 OCCURRENCE CODE DATE 37 36 CODE OCCURRENCE SPAN FROM THROUGH 36 CODE OCCURRENCE SPAN FROM THROUGH 38 39 40 41 VALUE CODES AMOUNT VALUE CODES AMOUNT VALUE CODES AMOUNT al b d 42 REY.CL. 43 DESCRIPTION 64 HCPCS / RATE/HIPPS COOE 45 BERK DATE 47 TOTAL CHARGES 48 NON COVERED CHARGES 49 110 1250 1258 + 270 271 272 1278 300 *310 10312 11360 - 370 1636 14710 MEDICAL SURGICAL PHARMACY IV SOLUTIONS MEDICAL SURGICAL SUPPLIES NON-STERILE SUPPLIES STERILE SUPPLIES IMPLANTS LABORATORY PATHOLOGY LAB PATHOLOGY/HISTOLOGY OR SERVICES ANESTHESIA DRUGS/DETAIL CODING REQUIRED RECOVERY ROOM 4 SERV. UNITS 8 240 6 300 35 2 2 1 48000.00 9500.59 2000.00 3500.00 6250.00 500.00 52169.00 1200.00 6000.00 4300.00 8000.00 511.00 6535.00 3775.00 10 11 12 8 4 300 5 + 9 13 14 16 16 10 16 17 IT 16 10 16 19 20 21 21 OF CREATION DATE PAGE 50 PAYER NAME Metropolitan HMO TOTALS 152240.59 55 EST AMOUNT DUE 56 NP 1354681526 51 HEALTH PLAN ID RU O ARO BEN, 54 PAIOR PAYMENTS 57 OTHER PRVID SORREO INSURE'S UNIQUE ID 61 GROUP NAME 62 INSURANCE GROUP NO. 58 INSURED'S NAME Jon Dough 68 TREATMENT AUTHORIZATION CODES 64 DOCUMENT CONTROL NUMBER 85 EMPLOYER NAME 59RFEINSURES UNIQUE ID 61 GROUP NAME 62 INSURANCE GROUP NO 58 INSURED'S NAME Jon Dough 68 TREATMENT AUTHORIZATION CODES 64 DOCUMENT CONTROL NUMBER 85 EMPLOYER NAME CA DA 68 87 C 73 CODE 245 72 ECI 7 PPS OTHER PROCEDURE CODE DATE b. 76 ATTENDING 69 ADMIT 70 PATIENT DX REASON DX 74 PRINCIPAL PROCEDURE A. OTHER PROCEDURE CODE DATE CODE DATE OJH608Z 04/02/2017 C. OTHER PROCEDURE d. OTHER PROCEDURE CODE DATE CODE DATE NFI QUAL FAST LASI CODE OTHER PROCEDURE DATE 77 OPERATING NAI QUAL LAST FIRST 80 REMARKS 8100 78 OTHER QUAL b LAST FEST G 79 OTHER NA CUAL LAST FIRST THE CERTIFICATIONS ON THE REVERSE APPLY TO THIS BILL AND ARE MADE A PART HEREOF. UB-04 CMS-1460 APPROVED OMB NO. 0938-0997 NUBC Triage Hospital 221 Main St Suite 1100 San Francisco, CA 94105 CNTL b. MED REC. S FED. TAX NO. OF BILL 131 Example 2 - Account #62 6 STATEMENT COVERS PERIOD FROM THROUGH 4/3/2017 4/4/2017 S PATIENT NAME Doug Overpayment 9 PATENT ADDRESS CONDITION CODES 22 24 29 ACDT 30 21 27 STATE 10 BIRTHDATE 08/18/1964 31 OCCURRENCE COOF DATE 11 SEX ADMISSION 12 DATE 13 HA 14 TYPE 15 SRO 16 DHR17 STAT 18 18 04/03/2017 01 32 OCCURRENCE 33 OCCURRENCE 34 CODE OCCURRENCE DATE DATE CODE DATE 36 37 36 CORE OCCURRENCE SPAN FROM THROUGH CODE OCCURRENCE SPAN FROM THROUGH et 3A 19 41 VALUE CODES AMOUNT 40 CODE VALUE CODES AMOUNT CODE VALUE CODES AMOUNT a b d 4 HCPCS / RATE/HIPPS CODE 45 BERK DATE 48 NON COVERED CHARGES 49 12 REY.CO. 45 DESCRIPTION 250 PHARMACY 1278 IMPLANTS 1481 CATH LAB +1 710 RECOVERY ROOM 4 SERV. UNITS 25 2 7 5 47 TOTAL CHARGES 5512.54 10680.00 34000.00 30950.11 93501 3 2 'N 10 111 11 1E 12 15 14 14 TE 15 10 16 151 16 10 15 19 20 20 21 21 OF CREATION DATE PAGE 50 PAYER NAME TOTALS 53287.65 55 EST AMOUNT DUE 56 NPI 1354681526 ROL SARO 51 HEALTH PLAN ID 54 PAIOR PAYMENTS Metropolitan HMO 57 OTHER PRVID 58 INSURED'S NAME 59RRE. BINSURED'S UNIQUE ID 61 GROUP NAM 62 INSURANCE GROUP NO. Doug Overpayment 68 TREATMENT AUTHORIZATION CODES 64 DOCUMENT CONTROL NUMBER 85 EMPLOYER NAME 68 100 IDB TIPPS 69 ADMIT DX 74 70 PATIENT REASON DX PRINCIPAL PROCEDURE Tr CODE 72 ECI OTHER PROCEDURE oor DATE b. OTHER PROCEDURE CODE 76 ATTENDING NAI QUAL Triage Hospital 221 Main St Suite 1100 San Francisco, CA 94105 3a PAT, CNTL b. MLD AFC. 4 TYPE OF BILL 111 Account #54 7 S FED. TAX NO. 6 STATEMENT COVERS PERIOD FROM THROUGH 12/1/2017 12/8/2017 S PATIENT NAME Tom Montana 9 PATIENT ADDRESS 11 SEX 12 21 CONDITION CODES 22 23 24 27 28 29 ACDT 30 STATE 10 BIRTHDATE 01/20/1950 31 OCCURRENCE COOF DATE ADMISSION DATE 13 R 14 TYPE 15 SRO 18 DHR17 STAT 18 18 12/01/2017 003 1 11 01 32 OCCURRENCE 33 OCCURRENCE 34 CODE OCCURRENCE DATE DATE CODE DATE 37 CODE 36 COCE OCCURRENCE SPAN FROM THROUGH 36 COOF OCCURRENCE SPWN FROM THROUGH 3 19 CORE al VALUE CODES AMOUNT 40 CODE VALUE CODES AMOUNT 41 CORE VALUE CODES AMOUNT b c d 42 REY.CO. 64 HCPCS / RATE/HIPPS COOE 45 BERN DATE 18 SERV, UNITS 48 NON-COVERED CHARGES 49 110 250 -258 4270 271 272 7 278 .300 310 10312 1360 15370 1636 14710 43 DESCRIPTION MEDICAL SURGICAL PHARMACY IV SOLUTIONS MEDICAL SURGICAL SUPPLIES NON-STERILE SUPPLIES STERILE SUPPLIES IMPLANTS LABORATORY PATHOLOGY LAB PATHOLOGY/HISTOLOGY OR SERVICES ANESTHESIA DRUGS/DETAIL CODING REQUIRED RECOVERY ROOM 7 240 6 250 35 2 2 1 4 3 8 4 300 5 47 TOTAL CHARGES 42000.00 5500.59 1000.00 4411.00 6250.00 500.00 42258.00 1200.00 2000.00 4300.00 4000.00 511.00 5535.00 3775.00 111 12 14 TE lis 1 lig 171 16 lig 15 19 20 211 21 OF PAGE 50 PAYER NAME Metropolitan HMO CREATION DATE ABO 54 PAIOR PAYMENTS TOTALS 123240.59 55 EST. AMOUNT DUE 56 NP 1354681526 51 HEALTH PLAN ID 57 OTHER PRVID INSURANCE GROUP NO. SORREO INSURED'S UNIQUE ID 61 GROUP NAME 58 INSURED'S NAME Tom Montana 63 TREATMENT AUTHORIZATION CODES 64 DOCUMENT CONTROL NUMBER 85 EMPLOYER NAME CA DA 68 TIPPS 69 ADMIT DX 74 73 70 PATIENT REASON DX PRINCIPAL PROCEDURE 72 ECI CODE 243 OTHER PROCEDURE b. OTHER PROCEDURE 'Triage Hospital 221 Main St Suite 1100 San Francisco, CA 94105 3a PAT. CNTL b.MED. RFC. 4 TYPE OF BILL 131 Account #63 6 S FED. TAX NO. STATEMENT COVERS PERIOD FROM THROUGH 5/17/2017 5/17/2017 S PATENT NAME Vivian Variance 9 PATENT ADDRESS CONDITION CODES 22 22 21 25 27 29 ACDT 30 STATE 28 10 BIRTHDATE 03/22/1976 31 OCCURRENCE COOF DATE 11 SEX ADMISSION 12 DATE 13 PR 14 TYPE 15 SRC 16DHR 17 STAT 18 10 05/17/2017 01 32 OCCURRENCE 33 OCCURRENCE 34 CODE OCCURRENCE DATE COOF DATE CODE DATE 37 36 COCE OCCURRENCE SPAN FROM THROUGH 36 COOF OCCURRENCE SPAN FROM THROUGH et 38 19 VALUJE CODES AMOUNT 40 COLE VALUE CODES AMOUNT 41 CORE VALLIE CODES AMOUNT a b d 42 REV.CD 44 HCPCS / RATE/HIPPS COOL 45 BERK DATE 4a NONCOVERED CHARGES 49 250 1335 636 4710 43 DESCRIPTION PHARMACY CHEMOTHERAPY/IV DRUGS/DETAIL CODE RECOVERY ROOM 48 SERV. UNITS 3 8 200 1 47 TOTAL CHARGES 200.00 3500.00 57840.00 1000.00 J9299 5 2 10 11 111 15 12 1E 13 14 14 TE 15 10 16 17 10 10 15 19 20 20 21 21 OF PAGE 50 PAYER NAME Metropolitan HMO CREATION DATE REL PO , 54 PAIOR PAYMENTS 51 HEALTH PLAN ID TOTALSI 62540.00 55 EST AMOUNT DUE 56 NP 1354681526 57 OTHER PRVID SORRE COINSURED'S UNIQUE ID 61 GROUP NAME 6 INSURANCE GROUP NO. 58 INSURED'S NAME Vivian Variance 69 TREATMENT AUTHORIZATION CODES 64 DOCUMENT CONTROL NUMBER 85 EMPLOYER NAME A D 68 06 DO A 69 ADMIT 772 70 PATIENT BEACONY 73 71 PPE cond suite Account #57 AFC. S FED, TAX NO 6 San Francisco, CA 94105 STATEMENT COVERS PERIOD FROM THROUGH 11/1/2017 12/6/2017 & PATIENT NAME - Betsy Ross 9 PATENT ADDRESS 20 21 CONDITION CODES 22 23 24 27 28 29 ACDT 30 STATE 10 BIRTHDATE 05/25/1953 31 OCCURRENCE COOF DATE 11 SEX ADMISSION 12 DATE 13 H 14 TYPE IS SRO 10 DHR 1 STAT 18 18 11/01/2017 00 3 1 11 01 32 OCCURRENCE 33 OCCURRENCE 34 OCCURRENCE CODE DATE COOF DATE CODE DATE 36 37 OCCURRENCE SPAN FROM THROUGH 36 COOF OCCURRENCE SPAN FROM THROUGH et 3A 39 VALUE CODES AMOUNT 40 CODE VALUE CODES AMOUNT 41 CODE VALUE CODES AMOUNT a b d 43 DESCRIPTION 44 HCPCS / RATE / HIPPS COOE 45 BERK DATE 48 NONCOVERED CHARGES 40 12 REY.CO. 200 INTENSIVE CARE *250 PHARMACY 258 IV SOLUTIONS + 270 MEDICAL SURGICAL SUPPLIES 271 NON-STERILE SUPPLIES 272 STERILE SUPPLIES 278 IMPLANTS 300 LABORATORY 310 PATHOLOGY LAB 10312 PATHOLOGY/HISTOLOGY 11360 OR SERVICES 15370 ANESTHESIA 636 DRUGS/DETAIL CODING REQUIRED 14710 RECOVERY ROOM 15 48 SERV. UNITS 35 520 9 321 35 2 2 1 4 15 8 30 3250 5 47 TOTAL CHARGES 332500.00 16500.00 10000.00 4411.00 9250.00 3500.00 8600.00 5787.54 7000.00 53000.00 15000.00 12000.00 247466.00 3775.00 10 11 12 15 14 15 id 16 15 10 10 15 19 20 21 OF PAGE 50 PAYER NAME Metropolitan HMO CREATION DATE 54 PRIOR PAYMENTS 51 HEALTH PLAN D TOTALSI 728789.54 55 EST AMOUNT DUE 56 NP 1354681526 57 OTHER PRVID 58 INSURED'S NAME SORREO INSURED'S UNIQUE ID 61 GROUP NAME 2 INSURANCE GROUP NO. Betsy Ross 68 TREATMENT AUTHORIZATION CODES 64 DOCUMENT CONTROL NUMBER 85 EMPLOYER NAME 100 DO 68 TIPP 73 CODE 20 ECI IS 69 ADMIT 70 PATIENT DX REASON DX 74 PRINCIPAL PROCEDURE OTHER PROCEDURE CODE DATE CODE DATE B313YZZ 11/01/2017 03VG3DZ 11/01/2017 76 ATTENDING NAI QUAL b. OTHER PROCEDURE CODE DATE 02HV33Z 11/20/2017 LAST FIRST Triage Hospital 221 Main St Suite 1100 San Francisco, CA 94105 2a PAT. CNTL b. MED REG. S FED. TAX NO. 4 TYPE OF BILL 131 Account #61 7 6 STATEMENT COVERS PERIOD FROM THROUGH 12/1/2017 12/2/2017 S PATIENT NAME Frank Underpayment 9 PATENT ADDRESS 21 CONDITION CODES 22 23 24 27 28 29 ACDT 30 STATE 10 BIRTHDATE 09/14/1955 31 OCCURRENCE COOE DATE 11 SEX ADMISSION 12 DATE 131 14 TYPE 15 SRC 18 DHR 17 STAT 18 18 12/01/2017 101 32 OCCURRENCE 33 OCCURRENCE 34 OCCURRENCE CODE 14 CODEDATE CODE_DATE 37 COCE OCCURRENCE EPAN FROM THROUGH 36 COOF OCCURRENCE EPWN FROM THROUGH et 38 39 CODE a VALLE CODES AMOUNT 40 COLE VALUE CODES BAUMIT 41 CORE VALLE CODES AMOUNT b d 12 REX.CO. 4 HCPCS / RATE/HIPPS COOL 45 BERK DATE 4 SERV. UNITS 48 NONCOVERED CHARGES 49 27 250 278 481 + 710 45 DESCRIPTION PHARMACY IMPLANTS CATH LAB RECOVERY ROOM 47 TOTAL CHARGES 4512.54 12680.00 32500.00 2986.00 93525 2 10 10 11 1E 12 JE 13 14 14 11 15 1 16 17 IT 13 10 15 19 20 20 21 21 OF PAGE 50 PAYER NAME Metropolitan HMO CREATION DATE AR O sex 54 PRIOR PAYMENTS NARO TOTALSI 52678.54 55 EST. AMOUNT DUE 56 NPI 1354681526 51 HEALTH PLAN ID 57 OTHER PRVID 58 INSURED'S NAME SORREO INSURED'S UNIQUE ID 61 GROUP NAME 62 INSURANCE GROUP NO Frank Underpayment 63 TREATMENT AUTHORIZATION CODES 64 DOCUMENT CONTROL NUMBER 85 EMPLOYER NAME 100 ID 68 69 ADMIT 70 PATIENT 7IPPS 72 TE Explanation of Benefits - Account #54 Patient Name Tom Montana Account 54 ID A11332211 Plan Dates of Service Metropolitan HMO 12/1/2017 - 12/8/2017 Excluded Disallowed Allowed Amount 23,800.00 Patient Responsibility 500.00 Benefit Paid 23,200.00 Expenses 110 42,000.00 278 42,258.00 Other 38,982.59 Total 123,240.59 42,258.00 38,982.59 38,982.59 23,800.00 42,258.00 500.00 23,300.00 Explanation of Benefits - Account #63 Patient Name Vivian Variance Account 63 ID A99955599 Plan Dates of Service Metropolitan HMO 5/17/2017 - 5/17/2017 Disallowed Expenses Other 62,540.00 Total 62,540.00 Excluded 62,540.00 62,540.00 Allowed Amount 39,894.27 39,894.27 Patient Responsibility Benefit Paid 1,000.00 38,894.27 1,000.00 38,894.27