Introduction:
A physician office (private practice) approached you in an effort to convert their paperwork process into a health information database. The physician provided a copy of the paperwork used in the office to collect patient information. The physician also explained the need to secure patient information and provided a list of the required level of access for each employee. Additional information will be provided upon request.
The physician would like to add to patient records results from labs and imaging. In addition, the physician would like to link with a list of pharmacies in the area and send the patient prescription electronically. As a database expert, you will be developing a patient database and all required tables using relational database approach.
Requirement:
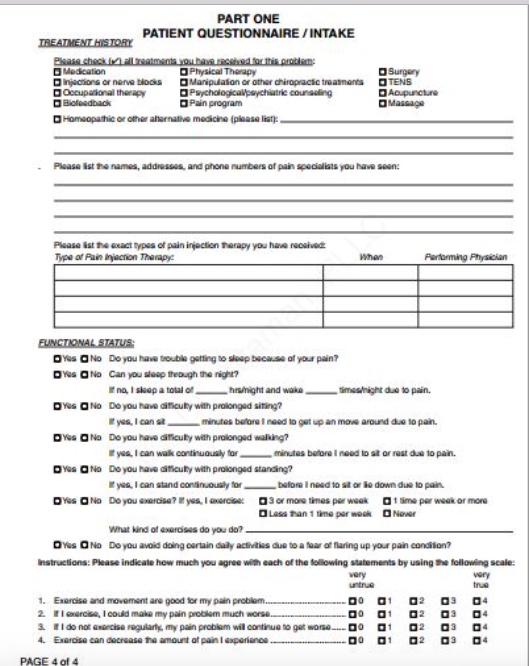
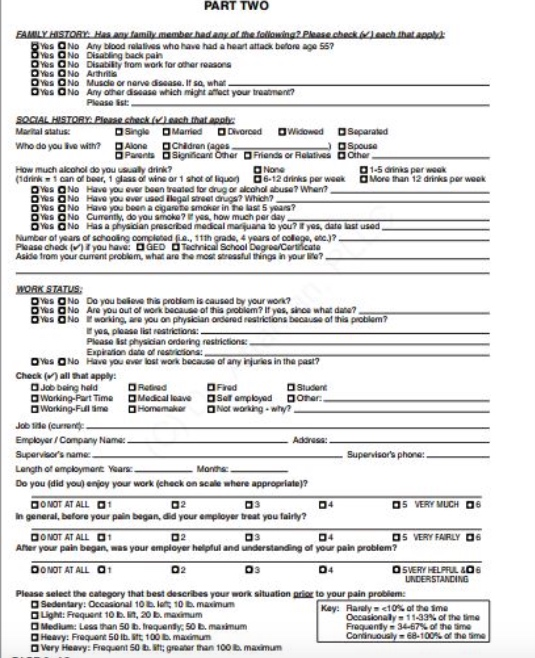
1.Analyze the provided forms below identifying the entities that should be tracked in the system.
2.Identify the fields (attributes) associated with each entity, listing possible candidate keys (determinants).
3.Based on your analysis and the given forms identify all possible functional dependencies (remember that those functional dependencies will not only assist in creating the proper tables but also will assist in understanding relationships between tables).
4.Create a separate entity to secure database with the list of required level access provided by the physician.
Forms and Documentation Provided:
The following are copies of the paper forms used in the office. Use these form to complete the assignment requirements above:
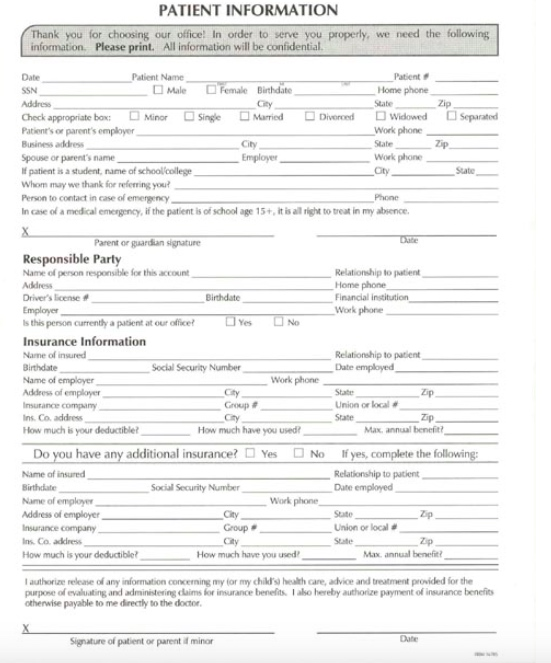



PATIENT INFORMATION k you for choosing our office! In order to serve you properly, we need the following information. Please print. All information will be confidential Patient Home phone Date Patient Name Male Female Birthdate Minor Single Mured DDiverod Dwidowed Work phone State Work phone Check appropriate box: Sparated Patient's or parent's employer Business address City patient is a student, name of schoollcollege Whom may we thank for referring you Person to contact in case of emergencoy In case of a medical emergency, if the patient is of school age 15+, it is al right to treat in my absence State- - Parent or gaardian signature Responsible Party Name of person responsible for this account Address Driver's leese # Emplayer s this Relationship to patient Home phone Financial institution Work phone Birthdate person currenthy a pasient at our office Insurance Information Name of insured Birthdate Name of employer Relationship to patient Date employed Social Security Number Work phone Address of employe Insurance company ns Co. address How much is your deductiblet Zip Group # Cty Union or local # State How much have you used Max, annual benefit Do you have any additional insurance? Yes Name of insured Birthdate Name of employe Address of employer Insurance company Ins Co. address How much is your deductible No If yes, complete the following: Relationship to patient Date employed Sociall Security Number Work phone City Group # City State Union or local # State Zp Max annual benefi How much have you used authorize release of any information concerning my for my child's health care, advice and treatment provided for the purpose of evalualting and administering claims for insurance benelits1 aso hereby authorize payment of insurance benefit otherwise payable to me direcly to the doctor. Signature of patient or parent if minor PART ONE PATIENT QUESTIONNAIRE/INTAKE aPhysical Therapy Surgery Dinjscions or nerve blooks Manipuiaion or othar chiropacic treatmens OTENS Pain program D Homsopathic or oher ahernatve medicine (plaase list Please ist he names, addresses and phone numbers of pain specialists you have seun Type of Pain injecnion Thempyc hen Parforming Physician Des O No Do you have ouble gattling to sap bacause of your pain? OYes aNo Do you have dificulty with prolonged siting? 0%:0No Doyou have dticuEy with prolonged waling? ta I can walk continuoualy formnes beforeineed to sit or rest due to pain. Do you ha dificuEy with prolonged standing? Yas a No yesI can stand coninuoualy for batore Ineed to sit or io down due to pain a Lesa han 1 time par wook ONower What kind a xerises do you do? Oes Q No Do you avoid doing certain daily activtss due to a foar of faring up your pain condiion? instructions: Please indicate how much agree with each ofthe tolowing statements by using the following scale: very vory . Exarcise and movement are good for my pain 2. Iercisa, I could make my pain problam much worse 1 02 3 04 PAGE 4 of 4 PART TWO ONo Any blood rolathes who have had a heart attack betore age 557 as ONo Disabling back pair O Yes QNo Disability from work for other reasons Oes ONo Muscle or nerve disease. If so, what Yas aNo Any oher dsease which migt auct your trea nen? Piease ist Marital status: Sing DMarried Divareed O Widowed Separated Who do you ive with? Aone D Chidren (ages Pasets Signicae Oher riends or Relatives Other How much alcohol do you usually drink? None 1-5 drinis per weok drink 1 can of bear,1 glaas af wine or 1 shot of liquon D6-12 drinks per weak Mone than 12 drinks per wook Yus a No Have you ever been realed og or akohal abuse? When? OYS ONo Have you ever used ilsgal setas? which? DYes ONo Havo you beon a cigarete smoker in he last 5 years? es ONo Cumently, do you smoka? yas how much per day Yes a No Has a physician prescribed medcal marquana to you? r yas, data ast used umber of years of schooling oomclaned 111h grade, 4 years ot colloa, ae) Please check )tyou have: DGED Tachnical School Degroa/Corticate Aside trom your curent problom wha are hmssul things in your li? es No Do you beliove this probiom is caused by your worn? No Are you out of work because of this probiam? If yes, sinoa whadae? Des aNo working,are you on physician ordured restrictions because of this problam? yos ploase list vestrictions Piease ist phyaician ordering restrictions Expiration date of resicions Have you ever lost work bacaw or any injuri s intr ows OND Check () all that apply: past? D Job being hald Fred a Sef employed a Working-Part Time Medical eave Doher Job tide (cuon Emplbyar / Campany Nama Supervisors name Langrh of amploymane years Do you (did you) enjoy your work (check on scale where appropriate)? Adonsa Su hone: Monte ONOT AT ALL O1 5 VERY MUCH 0 n general, before your pain bagan, did your employer treat you fairly? DONOT AT ALL1 S VERY FAIRLY Aner your pain began, was your employer helipful and understanding of your pain problem? DONOT AT ALL 1 02 UNDERSTANCING Please select the category that best deseribes your work situation ria to your pain protlem Sedentary: Occasional 10b lat 10 b. maximum Key: Raiuly, 2.5 Toxic> 30 Toxic> 20 Theophylline Tylenol Lithium 1.2 Toxic> 4000 mg/day CT Questionnaire Life. Well seen. Patient Name: Date: Referring Provider: What problems or complaints are you having that prompted your provider to order this test? How long have you had these symptoms? Have you had any other tests related to this problem or in this area of your body? Check all that apply: OCT Scan MRI Ultrasound Nuclear Medicine Scan x-ray Facility Were there any abnormalities? Have you ever received Intravenous Contrast/X-Ray dye? Are your Symptoms? MildModerate Severe Date(s): Yes No If yes, did you have an allergic reaction? If yes, please describe the reaction: Yes No Do you have or have you had in the past any of the following medical problems? (Check all that apply) Kidney problems/failure Stomach/Bowel Problems Urinary Tract Problems Heart Attack Irregular Heartbeat Diabetic and/or on metformin/metformin containing meds Cancer, where? Stroke Thyroid Problems Hepatitis High Blood Pressure requiring medication diagnosedTreatment ended(date)? Smoking History? YES NO If yes, for how many years? Packs per day? Please list any previous surgeries and/or any organs that were removed: Years since you quit (If applicable)? Is there a possibility that you are pregnant? For Staff Use Was the patient pre-medicated for this exam? YES NO Are you currently breastfeeding: YES NO Yes No Tech Notes/Initials PATIENT INFORMATION k you for choosing our office! In order to serve you properly, we need the following information. Please print. All information will be confidential Patient Home phone Date Patient Name Male Female Birthdate Minor Single Mured DDiverod Dwidowed Work phone State Work phone Check appropriate box: Sparated Patient's or parent's employer Business address City patient is a student, name of schoollcollege Whom may we thank for referring you Person to contact in case of emergencoy In case of a medical emergency, if the patient is of school age 15+, it is al right to treat in my absence State- - Parent or gaardian signature Responsible Party Name of person responsible for this account Address Driver's leese # Emplayer s this Relationship to patient Home phone Financial institution Work phone Birthdate person currenthy a pasient at our office Insurance Information Name of insured Birthdate Name of employer Relationship to patient Date employed Social Security Number Work phone Address of employe Insurance company ns Co. address How much is your deductiblet Zip Group # Cty Union or local # State How much have you used Max, annual benefit Do you have any additional insurance? Yes Name of insured Birthdate Name of employe Address of employer Insurance company Ins Co. address How much is your deductible No If yes, complete the following: Relationship to patient Date employed Sociall Security Number Work phone City Group # City State Union or local # State Zp Max annual benefi How much have you used authorize release of any information concerning my for my child's health care, advice and treatment provided for the purpose of evalualting and administering claims for insurance benelits1 aso hereby authorize payment of insurance benefit otherwise payable to me direcly to the doctor. Signature of patient or parent if minor PART ONE PATIENT QUESTIONNAIRE/INTAKE aPhysical Therapy Surgery Dinjscions or nerve blooks Manipuiaion or othar chiropacic treatmens OTENS Pain program D Homsopathic or oher ahernatve medicine (plaase list Please ist he names, addresses and phone numbers of pain specialists you have seun Type of Pain injecnion Thempyc hen Parforming Physician Des O No Do you have ouble gattling to sap bacause of your pain? OYes aNo Do you have dificulty with prolonged siting? 0%:0No Doyou have dticuEy with prolonged waling? ta I can walk continuoualy formnes beforeineed to sit or rest due to pain. Do you ha dificuEy with prolonged standing? Yas a No yesI can stand coninuoualy for batore Ineed to sit or io down due to pain a Lesa han 1 time par wook ONower What kind a xerises do you do? Oes Q No Do you avoid doing certain daily activtss due to a foar of faring up your pain condiion? instructions: Please indicate how much agree with each ofthe tolowing statements by using the following scale: very vory . Exarcise and movement are good for my pain 2. Iercisa, I could make my pain problam much worse 1 02 3 04 PAGE 4 of 4 PART TWO ONo Any blood rolathes who have had a heart attack betore age 557 as ONo Disabling back pair O Yes QNo Disability from work for other reasons Oes ONo Muscle or nerve disease. If so, what Yas aNo Any oher dsease which migt auct your trea nen? Piease ist Marital status: Sing DMarried Divareed O Widowed Separated Who do you ive with? Aone D Chidren (ages Pasets Signicae Oher riends or Relatives Other How much alcohol do you usually drink? None 1-5 drinis per weok drink 1 can of bear,1 glaas af wine or 1 shot of liquon D6-12 drinks per weak Mone than 12 drinks per wook Yus a No Have you ever been realed og or akohal abuse? When? OYS ONo Have you ever used ilsgal setas? which? DYes ONo Havo you beon a cigarete smoker in he last 5 years? es ONo Cumently, do you smoka? yas how much per day Yes a No Has a physician prescribed medcal marquana to you? r yas, data ast used umber of years of schooling oomclaned 111h grade, 4 years ot colloa, ae) Please check )tyou have: DGED Tachnical School Degroa/Corticate Aside trom your curent problom wha are hmssul things in your li? es No Do you beliove this probiom is caused by your worn? No Are you out of work because of this probiam? If yes, sinoa whadae? Des aNo working,are you on physician ordured restrictions because of this problam? yos ploase list vestrictions Piease ist phyaician ordering restrictions Expiration date of resicions Have you ever lost work bacaw or any injuri s intr ows OND Check () all that apply: past? D Job being hald Fred a Sef employed a Working-Part Time Medical eave Doher Job tide (cuon Emplbyar / Campany Nama Supervisors name Langrh of amploymane years Do you (did you) enjoy your work (check on scale where appropriate)? Adonsa Su hone: Monte ONOT AT ALL O1 5 VERY MUCH 0 n general, before your pain bagan, did your employer treat you fairly? DONOT AT ALL1 S VERY FAIRLY Aner your pain began, was your employer helipful and understanding of your pain problem? DONOT AT ALL 1 02 UNDERSTANCING Please select the category that best deseribes your work situation ria to your pain protlem Sedentary: Occasional 10b lat 10 b. maximum Key: Raiuly, 2.5 Toxic> 30 Toxic> 20 Theophylline Tylenol Lithium 1.2 Toxic> 4000 mg/day CT Questionnaire Life. Well seen. Patient Name: Date: Referring Provider: What problems or complaints are you having that prompted your provider to order this test? How long have you had these symptoms? Have you had any other tests related to this problem or in this area of your body? Check all that apply: OCT Scan MRI Ultrasound Nuclear Medicine Scan x-ray Facility Were there any abnormalities? Have you ever received Intravenous Contrast/X-Ray dye? Are your Symptoms? MildModerate Severe Date(s): Yes No If yes, did you have an allergic reaction? If yes, please describe the reaction: Yes No Do you have or have you had in the past any of the following medical problems? (Check all that apply) Kidney problems/failure Stomach/Bowel Problems Urinary Tract Problems Heart Attack Irregular Heartbeat Diabetic and/or on metformin/metformin containing meds Cancer, where? Stroke Thyroid Problems Hepatitis High Blood Pressure requiring medication diagnosedTreatment ended(date)? Smoking History? YES NO If yes, for how many years? Packs per day? Please list any previous surgeries and/or any organs that were removed: Years since you quit (If applicable)? Is there a possibility that you are pregnant? For Staff Use Was the patient pre-medicated for this exam? YES NO Are you currently breastfeeding: YES NO Yes No Tech Notes/Initials




