Problem 1: Using the study by Zare et al (2018)Influence of Adverse Childhood Experiences on Anxiety and Depression in Children Aged 6 to 11 years,
Problem 1:Using the study by Zare et al (2018)Influence of Adverse Childhood Experiences on Anxiety and Depression in Children Aged 6 to 11 years, provide answers to the following:
What is the purpose of this study?
Does this study address any gaps in current research as it relates to the topic?
Discuss the sample (e.g., data source, sample size, missing data) used in the analyses and measures (e.g., the dependent and independent variables)
What statistical methods did the researcher use to analyze the data and why?
What do the results show?
Describe the limitations of this study?
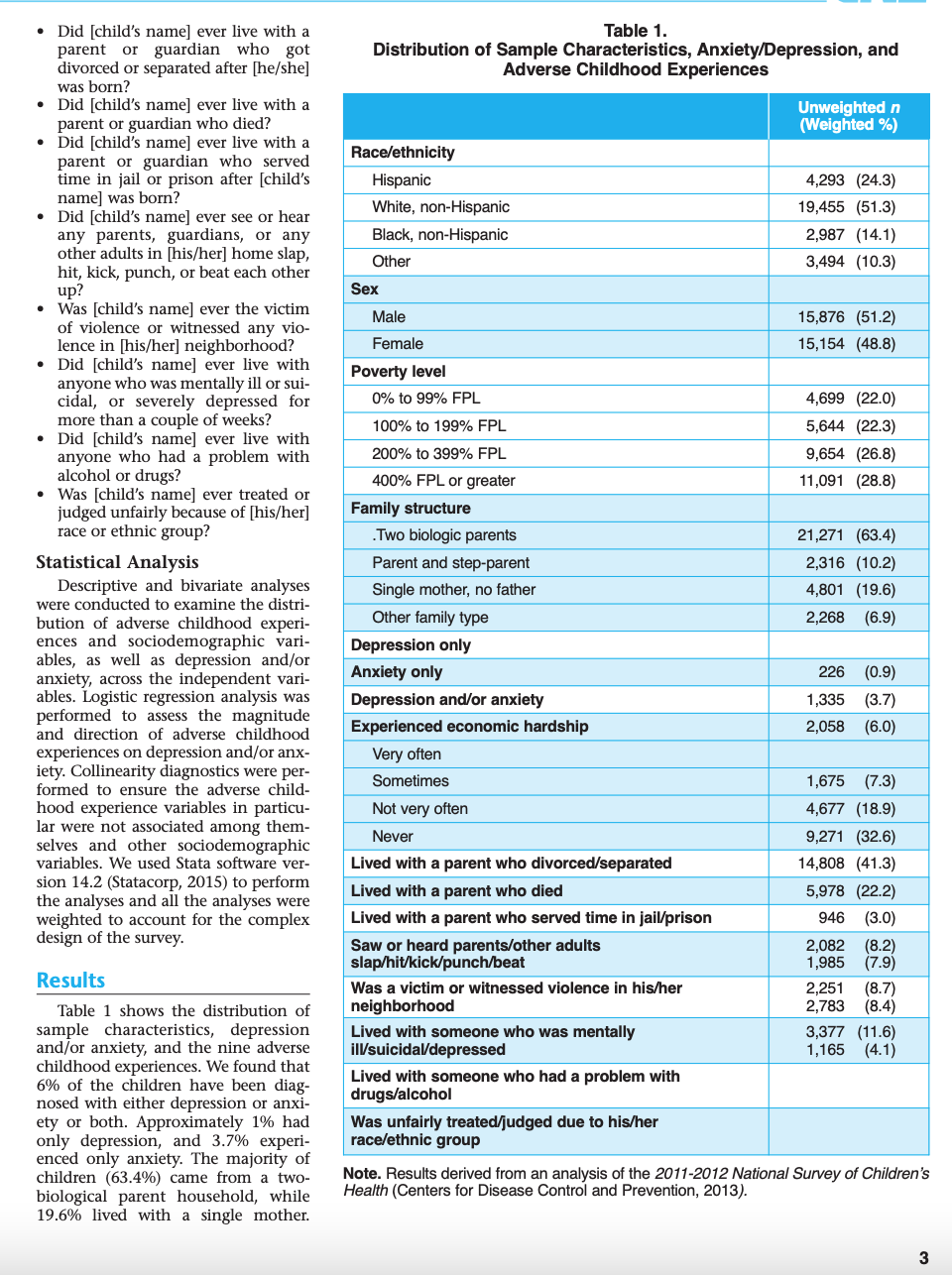
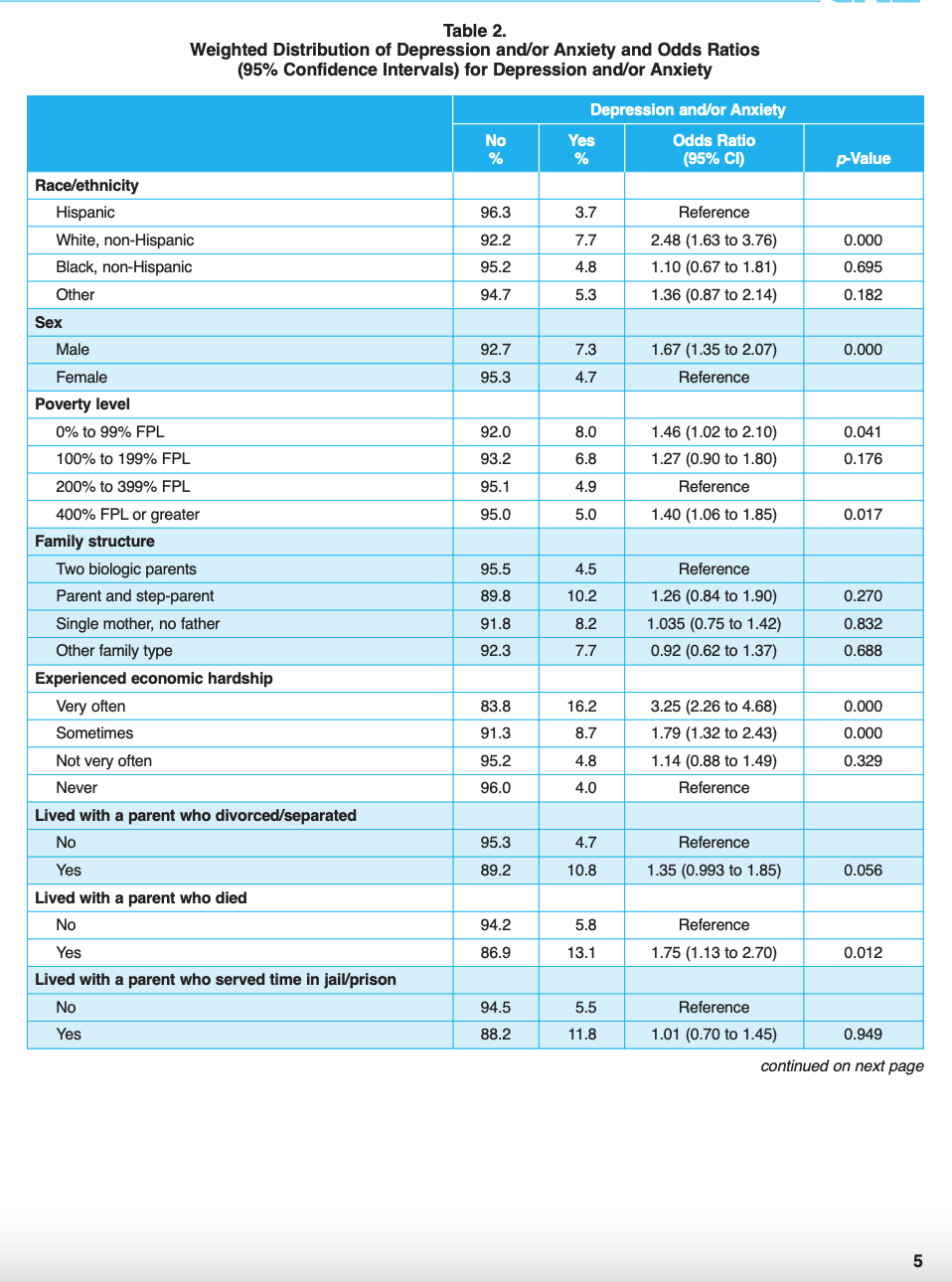
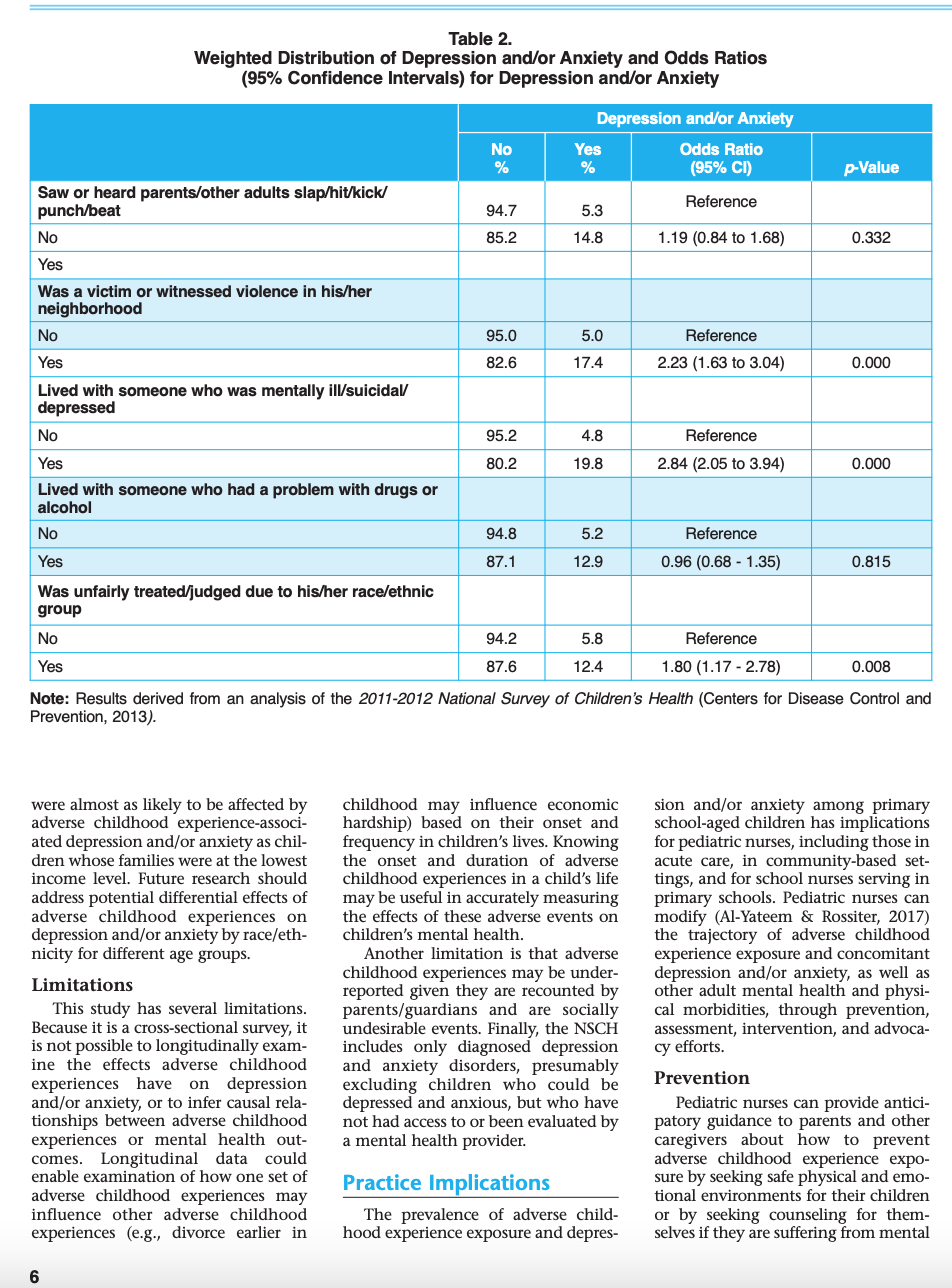
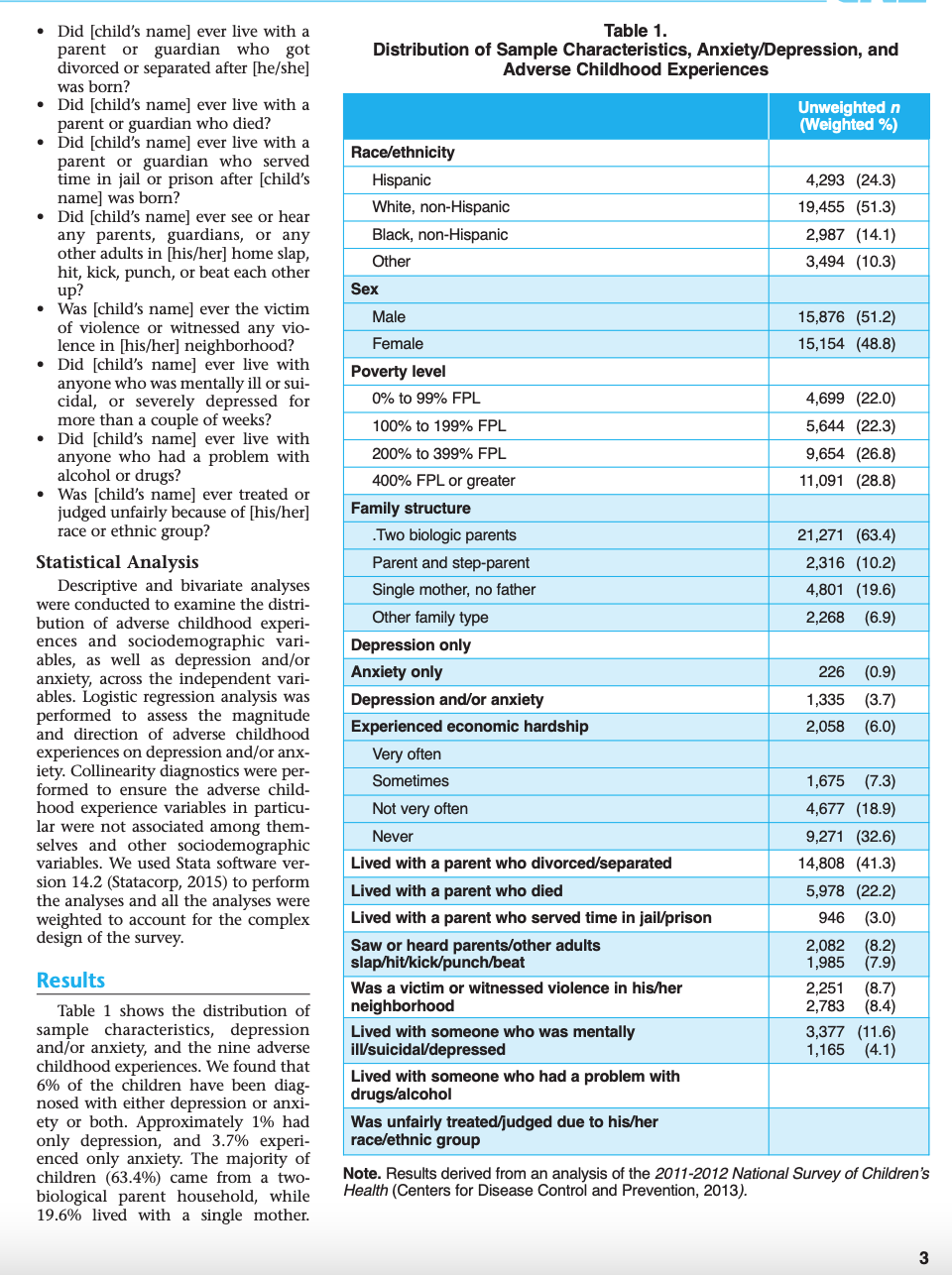
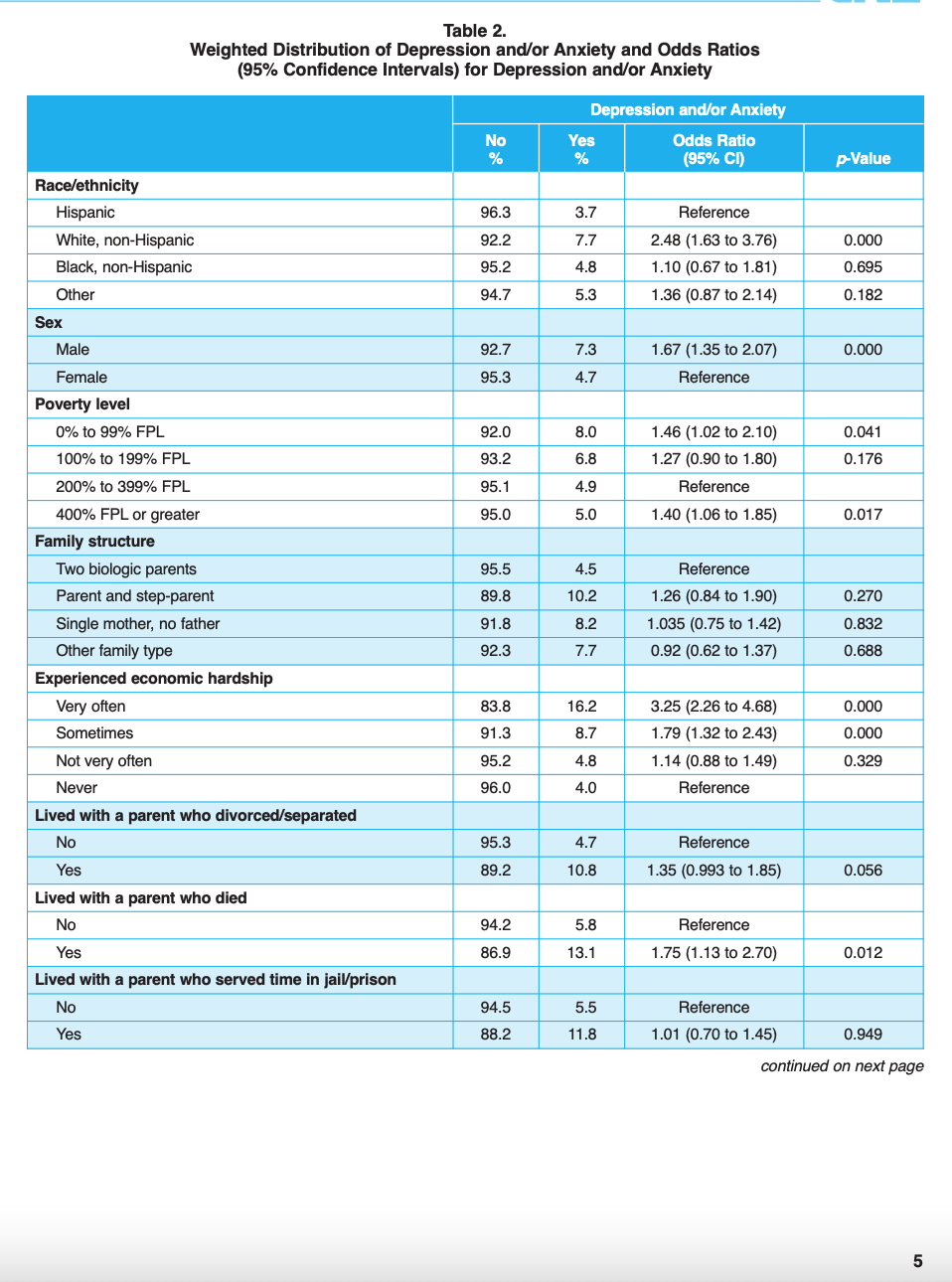
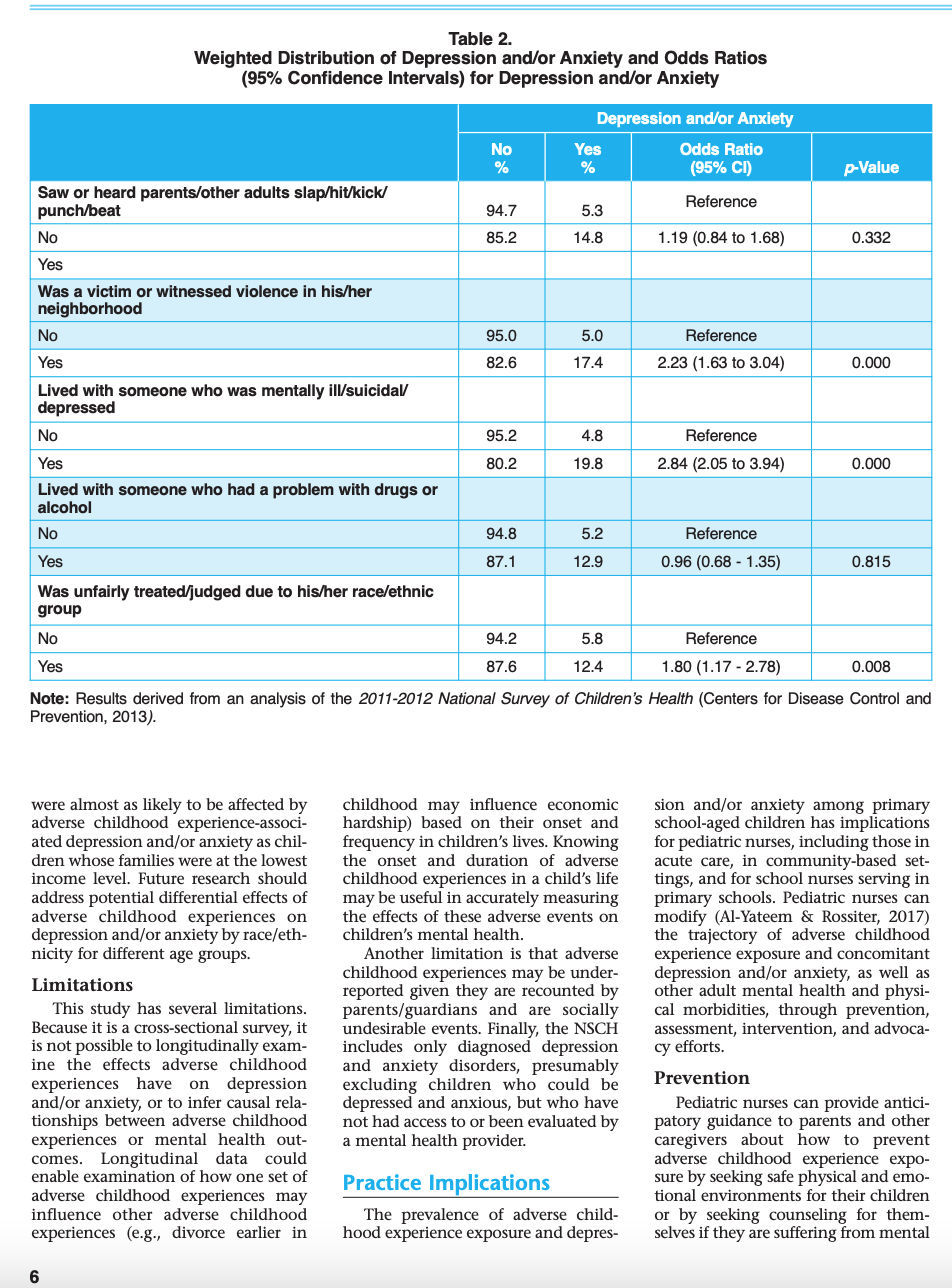
Influence of Adverse Childhood Experiences on Anxiety and Depression In Children Aged 6 to 11 Years Mojtaba Zare, Mary Narayan, Annie Lasway, Panagiota Kitsantas Janusz Wojtusiak, and Cheryl A. Oetjen P popular media, such as CBS' 60 Minutes (Winfrey, 2018) (AU: Zare, M., Narayan, M., Lasway, A., Kitsantas, P., Wojtusiak, J., & Oetjen, C.A. Please add to reference (2018). Influence of adverse childhood experiences on anxiety and depres- list.) and the PBS News Hour sion in children aged 6 to 11 years. Pediatric Nursing, 44(6), XXX-XXX Harris, 2018), have recently high- lighted the importance of addressing Adverse childhood experiences, such as exposure to poverty, violence, discrimina- the needs of children who have been ion, and prolonged parental absence, can cause toxic stress and can affect chil- negatively affected by adverse child- dren's physical, mental, and behavioral health for the rest of their lives. We exam- hood experiences. According to the ined the association of adverse childhood experiences with depression and anxiety American Academy of Pediatrics in the understudied population of children 6 to 11 years old. We performed a sec- (AAP), children affected by adverse ondary data analysis of the 2011/2012 National Survey of Children's Health. A sam- childhood experiences suffer from ple of 31,060 primary school-aged children was extracted from the nationally repre- "toxic stress," which is defined as sentative sample of 95,677 children 0 to 17 years old. Independent variables includ "excessive or prolonged activation of ed sociodemographic items related to the social determinants of health (race/eth- the physiologic stress response sys- nicity, sex, poverty level, family structure) and adverse childhood experience-expo- tems in the absence of the buffering sure items (family economic hardship, parental separation/divorce, parental incar- protection afforded by stable, respons ceration, parental/family member with mental illness or depression, parental/family sive relationships" (Garner member with drug or alcohol problem, and exposure to prejudice or discrimination). & Outcome variables were diagnosed depression and anxiety. Descriptive statistics Shonkoff, 2012, p. e225). When chil- and logistic regression analyses were performed. Findings showed that in this sam- dren experience prolonged physiolog- ple, 6% of children were diagnosed with depression and/or anxiety. Findings also ic stress responses, chemical and phys- showed that economic hardship, poor parental mental/behavioral health, exposure ical changes in children's neural net- to violence, or racial/ethnic discrimination increased the risk of depression and/or works and metabolic processes occur. anxiety in 6- to 11-year-old children. Pediatric nurses can help protect children from These changes are related to physical, adverse childhood experience exposure and can help them recover from these mental, behavioral, and developmen- events. Pediatric nurses can identify children at risk, provide parental anticipatory al damage, which affect children's guidance, make referrals for mental health services and community-based pro- future lives in profound ways, con- grams, protect children from traumatic medical events, and provide resilience edu tributing to life-long morbidity and cation/skill-building, which can alleviate the long-term effects of adverse childhood life-limiting mortality (Garner & experiences exposure. Shonkoff, 2012). Key Words: Adverse childhood experiences, depression, anxiety, mental health, toxic stress, National Survey of Children's Health. Mojtaba Zare, MS, is (AU: Please add title.), Department of Health Administration and Policy College of Health and Human Services, George Mason University, Fairfax, Adverse childhood experiences such as being separated from their par- VA. include a wide range of traumatic and ents and other social supports, and by Mary Narayan, MSN, RN, HHCNS-BC, is toxic events that occur during losing their homes and cherished pos- "AU: Please add title.), School of Nursing, childhood, such as man-made and nat- sessions (Barber, Kohl, Kassam-Adams, College of Health and Human Services, ural disasters, traumatic medical & Gold, 2014a; Quinn et al., 2016). George Mason University, Fairfax, VA. events, violence, discrimination, Witnessing or experiencing violent Annie Lasway, MS, is (AU: Please add poverty, dysfunctional families, and events (i.e., neighborhood violence, title.), Department of Health Administration tragic family events. Disasters may sexual violence, physical and psycho- and Policy, College of Health and Human cause children psychological trauma, logic abuse) is harmful to children Services, George Mason University, Fairfax, VA. Panagiota Kitsantas, PhD, is (AU: Please Janusz Wojtusiak, PhD, is (AU: Please add title.), Department of Health Administration and add title.), Department of Policy, College of Health and Human Services, George Mason University, Fairfax, VA. Administration and Policy, College of Health and Human Services, George Mason Cheryl A. Oetjen, DNP, FNP-BC, is (AU: Please add title.), School of Nursing, College of Health University, Fairfax, VA. and Human Services, George Mason University, Fairfax, VA.(Avanci, Assis, Oliveira, & Pires, 2012; (Avanci et al., 2012). Poor parental ing physical and mental health, access Blair, Mcfarlane, Nava, Gilroy, & mental health has been linked with to quality health care, and the child's Maddoux, 2015; Butler, Kowalkowski, mood/anxiety disorders and depres- family, neighborhood, school, and Jones, & Raphael, 2012). In addition, sion in young children (Lewis et al., social context" (Tufts University, racism and discrimination can also 2011; Reid, 2015). 2017). have long-term effects on children's A considerable number of research physical, mental, and behavioral studies has focused on adverse child- Sample health (Cooke, Bowie, & Carrere, hood experience-associated mental The NSCH was conducted using 2014; Garner & Shonkoff, 2012; Priest health problems in adolescents (12 to telephone numbers that were dialed at et al., 2013). 17 years old). Other studies have random to identify households with Other types of adverse childhood looked more broadly at the pediatric children under 18 years old. In total, experiences include living in poverty population, evaluating the effects on interviewers contacted 847,881 house- or living within families struggling to all children together, ages 2 through holds, of which 87,422 households meet basic physical needs, including 17 years, (Balistreri & Alvira- had age-eligible children, and inter- food and shelter, which can leave chil- Hammond, 2016; Barber et al., 2014; views were completed on 95,677 chil- dren with feelings of anxiety and sad- Bennett et al., 2012; Butler et al., dren (CDC, 2013). The sample for our ness (Butler et al., 2012). Separation 2012). To the best of our knowledge, analysis included only children from parents is traumatic for children, there is a gap in the literature about between the ages of 6 and 11 years. especially when it is permanent or the association between adverse child- This subsample included 31,060 chil- prolonged, such as when a parent dies hood experiences and depression dren. Missing data for the variables or is incarcerated, or when parents and/or anxiety in children 6 to 11 used in this study ranged from 0.06% divorce (Gjelsvi, Dumont, Nunn, & years old. to 2.4%. Rosen, 2014; Larson & Halfon, 2013). Emotional separation from parents, Purpose Measures such as when a parent is severely The outcome variable, namely depressed, mentally ill, or has sub- This secondary data analysis study depression and/or anxiety, was con- stance abuse problems, also has detri- attempts to answer the question, "In structed based on two questions found mental effects on children (Bennett, the population of United States chil- in the NSCH: "Has a doctor or other Brewer, & Rankin, 2012; Lewis, Rice, dren 6 to 11 years old, what is the rela- health professional ever told you that Harold, Collishaw, & Thapar, 2011; tionship between adverse childhood child's name] has depression prob- Mendes et al., 2012). experiences and anxiety and depres- lems?" and "Has a doctor or other Adverse childhood experience- sion." Findings from quantitative health professional ever told you that related physical, mental, and behav- studies are significant to pediatric [child's name] has anxiety problems?" ioral health problems that start in nurses because they are uniquely posi- If a response was "yes" to either of childhood and extend into adulthood tioned to help identify and intervene these questions, then the outcome are numerous. They include asthma; with primary school-aged children variable was classified as depression obesity; adult cardiovascular and pul- who suffer from adverse childhood and/or anxiety, indicating the child monary disorders; and mood, anxiety, experience exposure, and adverse has depression or anxiety or both. If and substance abuse disorders, among childhood experience-related depres- the response was "no" for both depres- others (Campbell, Walker, & Egede, sion and anxiety. Early intervention, sion and anxiety, then the outcome 2016; Garner & Shonkoff, 2012; especially with programs that build variable was coded as "no," indicating Merrick et al., 2017, Remigio-Baker, resilience, can enable children to over- the child had neither anxiety nor Hayes, & Reyes-Salvail, 2015; Sareen et come the harmful effects of these con- depression. al., 2013). In children, adverse child- ditions on their health and well-being Sociodemographic variables include hood experience exposure is strongly during childhood and into adoles- ed race/ethnicity (Hispanic, White associated with depression and anxi- cence and adulthood (Garner & non-Hispanic, Black non-Hispanic, and ety disorders (Avanci et al., 2012; Shonkoff, 2012; Lavoie, Pereira, & Other; "Other" includes Asian, Ameri- Balistreri & Alvira-Hammond, 2016; Talwar, 2016). can Indian, Native Alaskan, Native Barber et al., 2014; Butler et al., 2012). Hawaiian, Other Pacific Islander and Research evidence shows that adoles- Design and Methods multi-racial children), family structure cents (12 to 17 years old) who experi- (two biological parents, parent and ence a large number of adverse child- hood experiences are more likely to Design step-parent, single mother-no father, other family type), sex (male, female), experience poor physical and mental To answer the research question, and poverty level (0% to 99% Federal outcomes as compared to their coun- we conducted a secondary data analy- Poverty Level (FPL), 100% to 199% FPL, erparts with fewer reported adverse sis of the 2011/2012 National Survey 200% to 399% FPL, 400% FPL or childhood experiences (Balistreri & of Children's Health (NSCH). The pur- greater). The variable poverty level was Alvira-Hammond, 2016; Bhatta, pose of this survey instrument, spon- constructed based on household Champion, Young, & Loika, 2018). sored by the Centers of Disease income reported in the NSCH. The Further, in a study of low-income Control and Prevention (CDC), was to nine adverse childhood experiences Brazilian children 6 to 10 years old, collect national data on the health included: 10% of the children in their sample and well-being of children between 0 . How often has it been hard to get were depressed, and their depression and 17 years of age. The NSCH pro- by on your family's income, such as was associated with poverty and grow- vides rich data on "multiple, intersect- having enough money for basics ing up in dysfunctional families ing aspects of children's lives, include like food or housing?Did [child's name] ever live with a Table 1. parent or guardian who got Distribution of Sample Characteristics, Anxiety/Depression, and divorced or separated after [he/she] Adverse Childhood Experiences was born? Did [child's name] ever live with a Unweighted n parent or guardian who died? Weighted %) Did [child's name] ever live with a parent or guardian who served Race/ethnicity time in jail or prison after [child's Hispanic 4,293 (24.3) name] was born? Did [child's name] ever see or hear White, non-Hispanic 19,455 (51.3) any parents, guardians, or any Black, non-Hispanic 2,987 (14.1) other adults in [his/her] home slap, Other 3,494 (10.3) hit, kick, punch, or beat each other up? Sex Was [child's name] ever the victim Male 15,876 (51.2) of violence or witnessed any vio- lence in [his/her] neighborhood? Female 15,154 (48.8) Did [child's name] ever live with Poverty level anyone who was mentally ill or sui- cidal, or severely depressed for 0% to 99% FPL 4,699 (22.0) more than a couple of weeks? 100% to 199% FPL 5,644 (22.3) Did [child's name] ever live with anyone who had a problem with 200% to 399% FPL 9,654 (26.8) alcohol or drugs? 400% FPL or greater 11,091 (28.8) Was [child's name] ever treated or judged unfairly because of [his/her] Family structure race or ethnic group? .Two biologic parents 21,271 (63.4) Statistical Analysis Parent and step-parent 2,316 (10.2) Descriptive and bivariate analyses Single mother, no father 4,801 (19.6) were conducted to examine the distri- bution of adverse childhood experi- Other family type 2,268 (6.9) ences and sociodemographic vari- Depression only ables, as well as depression and/or anxiety, across the independent vari- Anxiety only 226 (0.9) ables. Logistic regression analysis was Depression and/or anxiety 1,335 (3.7) performed to assess the magnitude and direction of adverse childhood Experienced economic hardship 2,058 (6.0) experiences on depression and/or anx- Very often iety. Collinearity diagnostics were per- formed to ensure the adverse child- Sometimes 1,675 (7.3) hood experience variables in particu- Not very often 4,677 (18.9) lar were not associated among them- selves and other sociodemographic Never 9,271 (32.6) variables. We used Stata software ver- Lived with a parent who divorced/separated 14,808 (41.3) sion 14.2 (Statacorp, 2015) to perform the analyses and all the analyses were Lived with a parent who died 5,978 (22.2) weighted to account for the complex Lived with a parent who served time in jail/prison 946 (3.0) design of the survey. Saw or heard parents/other adults 2,082 (8.2) slap/hit/kick/punch/bea 1,985 (7.9) Results Was a victim or witnessed violence in his/her 2,251 (8.7) Table 1 shows the distribution of neighborhood 2,783 (8.4) sample characteristics, depression Lived with someone who was mentally 3,377 (11.6) and/or anxiety, and the nine adverse ill/suicidal/depressed 1,165 (4.1) childhood experiences. We found that 6% of the children have been diag- Lived with someone who had a problem with nosed with either depression or anxi- drugs/alcohol ety or both. Approximately 1% had Was unfairly treated/judged due to his/her only depression, and 3.7% experi- race/ethnic group enced only anxiety. The majority of children (63.4%) came from a two- Note. Results derived from an analysis of the 2011-2012 National Survey of Children's biological parent household, while Health (Centers for Disease Control and Prevention, 2013). 19.6% lived with a single mother.Male and female children were almost never lived with a parent or guardian lence and living with adults who have equally represented in the sample who died. The likelihood of depression mental health problems have been (51.2% and 48.8%, respectively). Most and/or anxiety was also higher among associated in prior research with poor of the children were White non- children who experienced or witnessed health and emotional problems in Hispanic (51.30%), followed by any violence in their neighborhoods children (Balisteri & Hammond, 2015; Hispanic (24.30%), Black non- (OR = 2.33, 95% CI = 1.63 to 3.04) or Bennett et al., 2012; Butler et al., Hispanic (14.10%), and Other (10.30 were ever treated or judged unfairly 2012). For example, poor parental %;). A large percentage of children because of race or ethnicity (OR = 1.80, mental health increased the preva- (44.3%) lived in households at or 95% CI = 1.17 to 2.78). Further, chil- lence of mental health conditions in below 199% of the FPL. dren who had lived with anyone with children 2 to 17 years old (Bennett et Regarding adverse childhood expe mental illness for more than a couple al., 2012). Low neighborhood support riences, 26.1% of the children's fami- of weeks were almost 3.0 (2.05 to 3.94) and poor physical qualities have also lies reported it was hard to afford basic times more likely to have depression been associated with higher depression life necessities. Also, 22.2% of the chil- and/or anxiety compared to children and/or anxiety in children 6 to 17 dren lived with a parent who separated who never lived in a similar situation. years old (Butler et al., 2012). Research or divorced after the child were born. evidence shows that stress may alter Although the majority of the sample Discussion hormone activity in children 97%) had not lived with a parent or Shonkoff & Garner 2012) that can guardian who died, 8.2% of the chil- The unique contribution of this trigger emotional distress (Sacks, dren lived with parents who served in analysis is that it elucidates and quan- Murphey & Moore, 2014), leading to jail or prison. Almost 8% of children tifies the effect of a set of adverse child- mental disorders, such as depression witnessed parent/adult physical abuse, hood experiences on depression and anxiety. while about 9% were victims of vio- and/or anxiety in a nationally repre- Sociodemographic factors were lence or witnessed neighborhood vio- sentative sample of 6- to 11-year old associated with depression and/or anx- lence. Further, 8.4% of these children children. We found that approximate- iety. In our sample of 6- to 11-year-old lived with someone who had a mental ly 1% of the sample were diagnosed children, boys were almost twice as health condition for more than two with depression (not anxiety), and likely as girls to be diagnosed with weeks, and 11.6% of children lived 3.7% were diagnosed with anxiety (not these disorders. This finding is not with parents who had abused alcohol depression), with a combined depres- consistent with previous research that or drugs. The majority of children sion and/or anxiety incidence of 6%. has focused on adolescents (13 to 17 (95.9%) did not experience racial/eth- Although in this study, depression was years old). For example, Kessler, nic discrimination. slightly lower than estimates reported Petukhova, Sampson, Zaslavsky and Findings related to bivariate and from a decade ago (depression at 1.4%) Wittchen (2012) found that females logistic regression analyses for depres- in 6- to 11-year-old children, anxiety are at higher risk for anxiety and sion and/or anxiety are shown in Table was considerable higher relative to depressive disorders compared to their 2. These findings show that White 2.9% from estimates reported about 10 male counterparts. This finding non-Hispanic children were 2.48 (1.63 years ago (Perou et al, 2013). Increases emphasizes the need for more research o 3.76) times more likely to experi- in depression and anxiety within in younger populations of children for ence depression and/or anxiety com- younger children in particular are con- depression and anxiety. Further, our pared to Hispanic children, while male cerning given their deleterious long- study shows that White (non- children were almost twice as likely to term effects on these children's well- Hispanic) children have the highest have depression and/or anxiety as being in adolescence and adulthood. It level of depression and/or anxiety, their female counterparts. Children also creates a substantial public health over twice the level for Hispanic chil- living in households at or less than problem within the context of limited dren. This is surprising given that 99% FPL and those at least 400% FPL mental health programs and resources. minority children are more likely to be were 40% to 46% times more likely to Further, findings of the present exposed to adverse childhood experi- have depression and/or anxiety com- study that primary school-aged chil- ences, such as racial/ethnic discrimina- pared to children from households dren are at risk for depression and/or tion, living in neighborhoods where with income levels between 200% and anxiety when exposed to adverse violence occurs, or being in families 399% FPL. childhood experiences are consistent unable to meet their food and shelter Analysis of adverse childhood exper with and extend previous research that needs (Priest et al., 2013). This finding rience factors indicated that children has examined the effects adverse child- may indicate that Hispanic children whose families "very often" and hood experiences on mental health in are more resilient to adverse childhood "sometimes" had difficulty affording the aggregate for U.S. children 2 to 17 experiences than White children. It basics, such as food or housing, were years old or adolescents 12 to 17 years could also mean their parents underre- 3.25 (2.26 to 4.68) and 1.79 (1.32 to old (Balistreri & Alvira-Hammond, port depression and/or anxiety due to 2.43) times more likely, respectively, to 2016; Bennett et al., 2012; Butler et al., cultural fears of stigmatization or that have depression and/or anxiety com- 2012). Particularly important con- Hispanic children lack access to the pared to children whose families tributing factors to depression and/or services that identify and treat chil- "never" had difficulties affording basic anxiety for 6- to 11-year-old children dren at risk, leading to underestima- necessities. Children who had lived include economic hardships, being tion of depression or anxiety in this with a parent or guardian who died victims of or exposed to violence, liv- group. Similarly, we found that fami- were at higher risk (OR = 1.75, 95% CI ing with someone who is mentally ill, lies at the highest income level, pre- = 1.13 to 2.70) for depression and/or and being treated unfairly because of sumably with the most resources to anxiety compared to children who their race/ethnicity. Exposure to vio- avoid adverse childhood experiences,Table 2. Weighted Distribution of Depression and/or Anxiety and Odds Ratios (95% Confidence Intervals) for Depression and/or Anxiety Depression and/or Anxiety No Yes Odds Ratio % (95% CD) p-Value Race/ethnicity Hispanic 96.3 3.7 Reference White, non-Hispanic 92.2 7.7 2.48 (1.63 to 3.76) 0.000 Black, non-Hispanic 95.2 4.8 1.10 (0.67 to 1.81) 0.695 Other 94.7 5.3 (0.87 to 2.14) 0.182 Sex Male 92.7 7.3 1.67 (1.35 to 2.07) 0.000 Female 95.3 4.7 Reference Poverty level 0% to 99% FPL 92.0 8.0 1.46 (1.02 to 2.10) 0.041 100% to 199% FPL 93.2 6.8 1.27 (0.90 to 1.80) 0.176 200% to 399% FPL 95.1 4.9 Reference 400% FPL or greater 95.0 5.0 1.40 (1.06 to 1.85) 0.017 Family structure Two biologic parents 95.5 4.5 Reference Parent and step-parent 89.8 10.2 1.26 (0.84 to 1.90) 0.270 Single mother, no father 91.8 8.2 1.035 (0.75 to 1.42) 0.832 Other family type 92.3 7.7 0.92 (0.62 to 1.37) 0.688 Experienced economic hardship Very often 83.8 16.2 3.25 (2.26 to 4.68) 0.000 Sometimes 91.3 B.7 1.79 (1.32 to 2.43) 0.000 Not very often 95.2 4.8 1.14 (0.88 to 1.49) 0.329 Never 96.0 4.0 Reference Lived with a parent who divorced/separated No 95.3 4.7 Reference Yes 89.2 10.8 5 (0.993 to 1.85) 0.056 Lived with a parent who died No 94.2 5.8 Reference Yes 86.9 13.1 1.75 (1.13 to 2.70) 0.012 Lived with a parent who served time in jail/prison No 94.5 5.5 Reference Yes 88.2 11.8 1.01 (0.70 to 1.45) 0.949 continued on next page 5Table 2. Weighted Distribution of Depression and/or Anxiety and Odds Ratios (95% Confidence Intervals) for Depression and/or Anxiety Depression and/or Anxiety No Yes Odds Ratio (95% CI) p-Value Saw or heard parents/other adults slap/hit/kick/ punch/beat 94.7 5.3 Reference No 85.2 14.8 1.19 (0.84 to 1.68) 0.332 Yes Was a victim or witnessed violence in his/her neighborhood No 95.0 5.0 Reference Yes 82.6 17.4 2.23 (1.63 to 3.04) 0.000 Lived with someone who was mentally ill/suicidal/ depressed No 95.2 4.8 Reference Yes 80.2 19.8 2.84 (2.05 to 3.94) 0.000 Lived with someone who had a problem with drugs or alcohol No 94.8 5.2 Reference Yes 87.1 12.9 0.96 (0.68 - 1.35) 0.815 Was unfairly treated/judged due to his/her race/ethnic group No 94.2 5.8 Reference Yes 87.6 12.4 1.80 (1.17 - 2.78) 0.008 Note: Results derived from an analysis of the 2011-2012 National Survey of Children's Health (Centers for Disease Control and Prevention, 2013) were almost as likely to be affected by childhood may influence economic sion and/or anxiety among primary adverse childhood experience-associ- hardship) based on their onset and school-aged children has implications ated depression and/or anxiety as chil- frequency in children's lives. Knowing for pediatric nurses, including those in dren whose families were at the lowest the onset and duration of adverse acute care, in community-based set- income level. Future research should childhood experiences in a child's life tings, and for school nurses serving in address potential differential effects of may be useful in accurately measuring primary schools. Pediatric nurses can adverse childhood experiences on the effects of these adverse events on modify (Al-Yateem & Rossiter, 2017) depression and/or anxiety by race/eth- children's mental health. the trajectory of adverse childhood nicity for different age groups. Another limitation is that adverse experience exposure and concomitant Limitations childhood experiences may be under- depression and/or anxiety, as well as reported given they are recounted by other adult mental health and physi- This study has several limitations. parents/guardians and are socially cal morbidities, through prevention, Because it is a cross-sectional survey, it undesirable events. Finally, the NSCH assessment, intervention, and advoca- is not possible to longitudinally exam- includes only diagnosed depression ry efforts. ine the effects adverse childhood and anxiety disorders, presumably experiences have on depression excluding children who could be Prevention and/or anxiety, or to infer causal rela- depressed and anxious, but who have Pediatric nurses can provide antici- tionships between adverse childhood not had access to or been evaluated by patory guidance to parents and other experiences or mental health out- a mental health provider. caregivers about how to prevent comes. Longitudinal data could adverse childhood experience expo- enable examination of how one set of Practice Implications sure by seeking safe physical and emo- adverse childhood experiences may tional environments for their children influence other adverse childhood The prevalence of adverse child- or by seeking counseling for them- experiences (e.g., divorce earlier in hood experience exposure and depres- selves if they are suffering from mentalInstructions For Continuing Nursing Education Contact Hours Influence of Adverse Childhood Experiences on Anxiety and Depression in Children Aged 6 to 11 Years Deadline for Submission: December 31, 2020 PED 1806 To Obtain CNE Contact Hours The author(s), editor, editorial board, 1. To obtain CNE contact hours, you must read the article and complete the evalu- content reviewers, and education director reported no actual or potential conflict of ation through the Pediatric Nursing website at www.pediatricnursing.net/ce interest in relation to this continuing nursing 2. Evaluations must be completed online by December 31, 2019. Upon completion education article. of the evaluation, your CNE certificate for 1.4 contact hour(s) will be mailed to This educational activity is provided by you. Anthony J. Jannetti, Inc. Anthony J. Jannetti, Inc. is accredited as a Learning Outcome provider of continuing nursing education by the American Nurses Credentialing Center's After completing this education activity, the learner will be able to identify the Commission on Accreditation. implications for pediatric nurses in helping to alleviate long term effects of adverse Anthony J. Jannetti, Inc. is a provider childhood experiences exposure. approved by the California Board of Registered Nursing, provider number CEP 5387. Licensees in the state of California must retain Learning Engagement Activity this certificate for four years after the CNE Download and review: activity is completed. Based on the results of the NSCH, identify the skills set necessary for the pediatric This article was reviewed and formatted for nurse to assess a child's exposure to adverse childhood experiences. contact hour credit by Rosemarie Marmion, MSN, RN-BC, NE-BC, Anthony J. Jannetti, Inc. Centers for Disease Control and Prevention. (2013). National survey of children's Education Director. health. Retrieved from http://www.cdc.govchs/slaitssch.htm Fees - Subscriber: FREE Regular: $20 health or substance abuse problems. needs and Supplemental Nutrition NSCH itself includes sensitive and Pediatric nurses can also advise parents Assistance Program (SNAP) for food well-tested parental questions about that they can help their children over- insecurities. exposure to many adverse childhood come the toxic stress of adverse experi- experiences, though not all of them ences by "being there;" providing love, Identification CDC, 2013). For instance, pediatric caring, and support as soon as possible Early identification enables early nurses could ask the questions about after such events; and not leaving chil- intervention. Children should be adverse childhood experience expo- dren alone to cope with their emotions screened for both adverse childhood sure identified earlier in the Measures and fears. Parents can help their chil- experience exposure, and for symp- section of this article. They could sup- dren cope with empathetic listening toms of anxiety and depression with plement these with additional ques- and by role-modeling constructive instruments designed for the children tions about adverse childhood experi- coping and resilience mechanisms themselves as well as for their parents. ences not investigated with the NSCH, (Garner & Shonkoff, 2012). When Each well child visit should follow the such as questions addressing child nurses encounter families whose chil- guidelines set forth by Bright Futures abuseeglect, natural disasters, and dren are at risk for adverse childhood (AAP, 2017). The children in this age traumatic medical events. Finally, the experiences (e.g., families living below group, referred to as middle child- lack of child-friendly screening tools the poverty line in violent neighbor- hood, are in a transitional period for adverse childhood experience hoods or parents who have not had where they are building the skills exposure beacons [AUTHOR: beck- good parental models themselves), the required to cope with stressors. ons?] nurse researchers to develop family can be referred to programs, Although the Bright Futures guidelines such instruments. such as Healthy Start, the Compre- for middle childhood do not include a hensive Child Development Program, formal tool for screening for depres- Intervention or the Nurse-Family Partnership Pro- sion, a priority for middle childhood Pediatric nurses may be the first to gram, which enable parents to adopt children includes addressing the social suspect a child has adverse childhood positive parenting techniques (Arrua- determinants of health, mental experience-associated depression and/ barrena & Paul, 2012; Garner & health, school, and safety. or anxiety. These nurses can alert the Shonkoff, 2012). Pediatric nurses are Screening tools have been devel- child's pediatrician or make referrals positioned to provide care coordina oped for older children and adults, but to mental health service programs. ion by referring parents to federal pro- screening tools for children age 6 to 11 They can also make referrals to their grams, such as Special Needs Assist- years need further development and organization's social workers or to ance Programs (SNAPS) for housing validation (AAP, 2014). However, the community-based programs, such asthe Big Brother/Big Sister programs. depression are associated with a life- Bhatta, S., Champion, J.D., Young, C., & Pediatric nurses can also learn how to time of mental, behavioral, and phys- Loika, E. (2018). Outcomes of depres- best promote resilience in these chil- ical problems. Compared to children sion screening among adolescents dren. The AAP and other organiza- who have not suffered from such accessing school-based pediatric pri- tions identify strategies that nurses mary care clinic services. Journal of problems, children who have experi- Pediatric Nursing, 38, 8-14. can use, such as promoting the 7Cs of enced adverse events have lower levels Blair, F., Mcfarlane, J., Nava, A., Gilroy, H., & Resilience (competence, confidence, of school/social success and higher Maddoux, J. (2015). Child witness to connectedness, character, contribu- levels of morbidity and early mortality domestic abuse: Baseline data analysis tion, coping, and control) or provid- throughout their lifespans. Pediatric or a seven-year prospective study. ing Trauma-Informed Care (Garner & nurses can help mitigate these prob- Pediatric Nursing, 41(1), 23-29. Shonkoff, 2012; Winfrey, 2018). Butler, A.M., Kowalkowski, M., Jones, H.A., & lems with interventions that help pre- Raphael, J.L. (2012). The relationship of Nurses can then educate parents, vent adverse childhood experience reported neighborhood conditions with teachers, coaches, and child care exposure, especially with parental child mental health. Academic providers on how they can be most anticipatory guidance. Nurses can also Pediatrics, 12(6), 523-531 helpful to these children. Nurses can alleviate adverse childhood experi- Campbell, J.A., Walker, R.J., & Egede, L.E. also use their empathic listening skills ence effects by identifying children (2016). Associations between adverse and their knowledge about how to who have been exposed to such childhood experiences, high-risk behav- iors, and morbidity in adulthood build resilience to directly provide the adverse events. They can then insti- American Journal of Preventive Medi- care these children need. Most impor tute interventions and referrals that cine, 50(3), 344-352. doi:10.1016/j. tantly, nurses can take steps to prevent help promote children's health and amepre.2015.07.022 current hospitalizations and medical well-being. Assessing a child's expo- Centers for Disease Control and Prevention. procedures from being traumatic for sure to adverse childhood experiences (2013). National survey of children's health. Retrieved from http://www.cdc. children with sensitive nursing inter- should be a key element of the nurse's govchs/slaitssch.htm ventions (Al-Yateem & Rossiter, 2017). assessment of children. Cooke, C.L., Bowie, B.H., & Carrere, S. (2014). Perceived discrimination and Advocacy children's mental health symptoms: Findings also emphasize the need References Advances in Nursing Science, 37(4), for public health policy and preven- Al-Yateem, N., & Rossiter, R.C. (2017). 299-314. https://doi.org/10.1097/ANS. 0000000000000047 tion programs that focus on family Unstructured play for anxiety in pediatric and community health and well- inpatient care: Journal for Specialists in Garner, A.S., & Shonkoff, J.P. (2012). Early Pediatric Nursing, 22(1), e12166. childhood adversity, toxic stress, and the being. Pediatric nurses can advocate doi:10.1111/jspn.12166 role of the pediatrician: Translating within their organizations, local American Academy of Pediatrics (AAP). developmental science into lifelong schools, and communities for strate- (2017). Bright futures: Guidelines for health. Pediatrics, 129(1), e224-e231. gies that promote child safety and health supervision of infants, children doi:10.1542/peds.2011-2662 environments that help children and adolescents (4th ed.). Itasca IL: Gjelsvik, A., Dumont, D.M., Nunn, A., & Rosen, D.L. (2014). Adverse childhood thrive, shielded from experiences that Author. events: Incarceration of household are detrimental to children's health Arruabarrena, I., & De Paul, J. (2012). Improving accuracy and consistency in members and health-related quality of and well-being throughout their child maltreatment severity assessment life in adulthood. Journal of Health Care entire lives. Finally, nurses can advo- in child protection services in Spain: or the Poor and Underserved, 25(3), cate for allocating resources for devel- New set of criteria to help caseworkers 1169-1182. doi:10.1353/hpu.2014.0112 oping mental health programs and n substantiation. Children and Youth Harris, N.B. (2018, February 26). Opinion: treatments as public health measures. Services Review, 34(4), 666-674. Too many children with toxic stress are Avanci, J., Assis, S., Oliveira, R., & Pires, T. being misdiagnosed. Retrieved from 2012). Childhood depression. Exploring https://www.pbs.orgewshour/health/op Conclusion the association between family violence nion-too-many-children-with-toxic- and other psychosocial factors in low- stress-are-being-misdiagnosed When young children's sense of income Brazilian schoolchildren. Child Kessler, R.C., Petukhova, M., Sampson, safety and security is threatened or and Adolescent Psychiatry and Mental N.A., Zaslavsky, A.M., & Wittchen, H.U. destroyed by traumatic events, such as Health, 6(1), 26. (2012). Twelve-month and lifetime Balistreri, K.S., & Alvira-Hammond, M. prevalence and lifetime morbid risk of natural disasters, parental separation, 2016). Adverse childhood experiences, anxiety and mood disorders in the violence, or other adverse events, chil- family functioning and adolescent health United States. International Journal of dren can be left with deep emotional and emotional well-being. Public Health, Methods in Psychiatric Research, 21(3), wounds that affect their mental 132, 72-78. doi:10.1016/j.puhe.2015. 169-184. doi:10.1002/mpr.1359 health. In this secondary data analysis 10.034 Larson, K., & Halfon, N. (2013). Parental divorce and adult longevity. International of the NSCH, the prevalence of diag- Barber, B.A., Kohl, K.L., Kassam-Adams, N., & Gold, J.I. (2014). Acute stress, Journal of Public Health, 58(1), 89-97. nosed anxiety and depression in chil- depression, and anxiety symptoms doi:10.1007/s00038-012-0373-x dren 6 to 11 years old exposed to among English and Spanish speaking Lavoie, J., Pereira, L.C., & Talwar, V. (2016). adverse childhood experiences is 6%. children with recent trauma exposure. Children's physical resilience outcomes: Many children exposed to these Journal of Clinical Psychology in Meta-analysis of vulnerability and pro- events may not have been adequately Medical Settings, 21(1), 66-71. doi:10. tective factors. Journal of Pediatric Nursing, 31(6), 701-711. doi:10.1016/ assessed by a pediatric provider skilled 1007/s10880-013-9382-Z Bennett, A.C., Brewer, K.C., & Rankin, K.M. .pedn.2016.07.011 in mental health assessment. The (2012). The association of child mental Lewis, G., Rice, F., Harold, G.T., Collishaw, prevalence of undiagnosed anxiety health conditions and parent mental S., & Thapar, A. (2011). Investigating and depression could be much higher. health status among U.S. children, environmental links between parent Resulting from exposure to adverse 2007. Maternal & Child Health Journal, depression and child depressive/anxiety childhood experiences, anxiety and 16(6), 1266-1275. doi:10.1007/s10995- symptoms using an assisted conception 011-0888-4 design. Journal of the American Aca
Step by Step Solution
There are 3 Steps involved in it
Step: 1
Get Instant Access to Expert-Tailored Solutions
See step-by-step solutions with expert insights and AI powered tools for academic success
Step: 2
Step: 3
Ace Your Homework with AI
Get the answers you need in no time with our AI-driven, step-by-step assistance