solve step by step with details using CMS-1500 form.
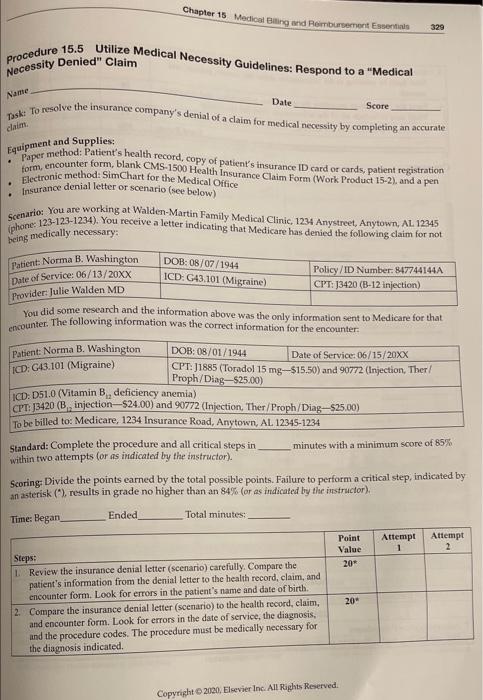
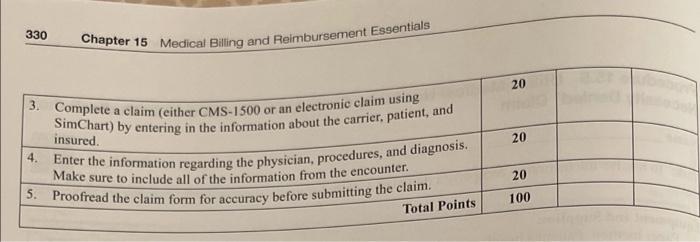
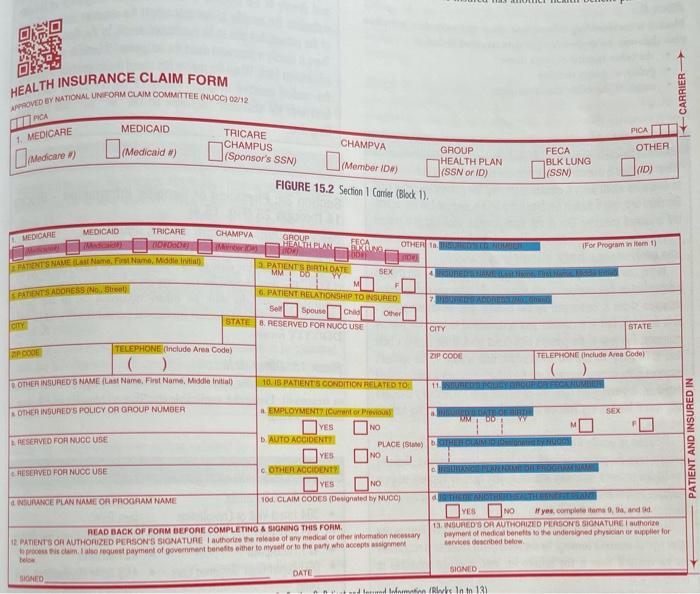
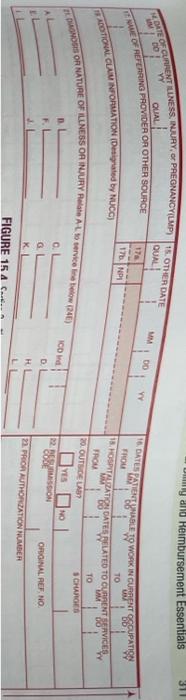
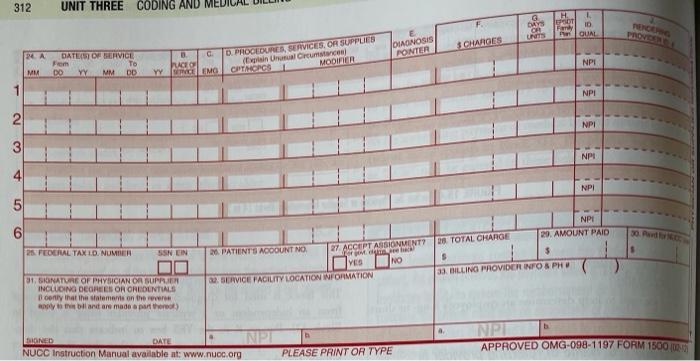
Chapter 15 Medical Biling and Rembursement Essentials 329 Procedure 15.5 Utilize Medical Necessity Guidelines: Respond to a "Medical Necessity Denied" Claim Name Date Poke to resolve the insurance company's denial of a claim for medical necesity by completing an accurate Score claim Equipment and Supplies . Paper method: Patient's health record, copy of patient's insurance ID card or cards, patient registration form, encounter form, blank CMS-1500 Health Insurance Claim Form (Work Product 15-2), and a pen Electronic method: SimChart for the Medical Office Insurance denial letter or scenario (see below) DOB: 08/07/1944 ICD: G43.101 (Migraine) Scenario: You are working at Walden-Martin Family Medical Clinic, 1234 Anystreet, Anytown, AL 12345 (phone: 123-123-1234). You receive a letter indicating that Medicare has denied the following claim for not being medically necessary: Patient: Norma B. Washington Date of Service: 06/13/20XX Policy/ID Number: 847744144A Provider: Julie Walden MD CPT: 13420 (B-12 injection) You did some research and the information above was the only information sent to Medicare for that encounter. The following information was the correct information for the encounter Patient Norma B. Washington DOB: 08/01/1944 Date of Service: 06/15/20XX ICD: G13.101 (Migraine) CPT: J1885 (Toradol 15 mg-$15.50) and 90772 (Injection, Ther/ Proph/Diag-525.00) ICDD51.0 (Vitamin B, deficiency anemia) CPT: 13420 (B, injection-$24.00) and 90772 (Injection, Ther/Proph/Diag-$25.00) To be billed to: Medicare, 1234 Insurance Road, Anytown, AL 12345-1234 Standard: Complete the procedure and all critical steps in minutes with a minimum score of 85% within two attempts (or as indicated by the instructor). Scoring: Divide the points earned by the total possible points. Failure to perform a critical step, indicated by an asterisk (*), results in grade no higher than an 84% (or as indicated by the instructor), a Time: Began Ended Total minutes Point Value 20 Attempt 1 Attempt 2 Steps: 1 Review the insurance denial letter (scenario) carefully. Compare the patient's information from the denial letter to the health record, claim, and encounter form. Look for errors in the patient's name and date of birth. 2. Compare the insurance denial letter (scenario) to the health record, claim, and encounter form. Look for errors in the date of service, the diagnosis, and the procedure codes. The procedure must be medically necessary for the diagnosis indicated, 20" Copyright 2020. Elsevier Inc. All Rights Reserved 330 Chapter 15 Medical Billing and Reimbursement Essentials 20 insured. 20 3. Complete a claim (either CMS-1500 or an electronic claim using SimChart) by entering in the information about the carrier, patient, and 4. Enter the information regarding the physician, procedures, and diagnosis. Make sure to include all of the information from the encounter. 5. Proofread the claim form for accuracy before submitting the claim. 20 100 Total Points FD HEALTH INSURANCE CLAIM FORM APPROVED BY NATIONAL UN FORM CLAIM COMMITTEE (NUCC) 0012 CARRIER BEROA 1. MEDICARE MEDICAID Dimo (Medicaid #) TRICARE CHAMPUS CHAMPVA PICABIE OTHER Medicare Sponsors SSN member 10 GROUP HEALTH PLAN FECA BLK LUNG (SSN) IND FIGURE 15.2 Section 1 Comer (Block 1). MEDICARE CHAMPVA MEDICAIC TRICARE no PATIENTS NAMEL Name. For me, Motor GROUP HETEN FECA PINO OTHER DUTER For Program in 1 3 PATIENTS BIRTH DATE W DO YY SEX EDIA SATIENTS ADORESSINS 6. PATIENT RELATIONSHIP TO INSURED Sell Soune CH Other STATE B. RESERVED FOR NUCCUSE CITY CITY STATE TELEPHONE (Include Area Code) ZIP COOL TELEPHONE (Include Area Code) OTHER INSURED'S NAME(Last Name First Name, Middle ) 10.IS PATIENTS CONDITION RELATED TO 11.NET OTHER INSURED'S POLICY OR GROUP NUMBER EMPLOYMENT DATE OF SEX WM DO YES NO RESERVED FOR NUOC USE D. AUTO ACCIDENT PLACE(S) OTHER CLAIM YES NO RESERVED FOR NUCC USE OTHER ACCOUNT VES ON SUNCE PLAN NAME OR PROCIRAM NAME 10d. CLAIM CODES (Designated by NUCC) Yes No If yes, cortoms and READ BACK OF FORM BEFORE COMPLETING & SIGNING THIS FORM 13. UNGURED'S OR AUTHORIZED PERSONS SIGNATURE I authorize IR PATIENTS OR AUTHORIZED PERSON'S SIGNATURE I authorize the release of any medical of the information costar payment of medical benefits to the undersigned physician or supplier for services described below is clamo request payment of government benefits other to myself or to the party who accepts diment PATIENT AND INSURED IN DATE SIONID BONEO Islami (wks in tn 13 my and Heimbursement Essentials 311 YY DO QUAL QUAL NOTE O CLIENTETINESS INUIRY, or PREGNANCYILMP16 OTHER DATE EGUE OF REFERRING PROVIDER OR OTHER SOURCE 8 09 178 17 FROM TO MEADOTIONAL CLAIM INFORMATION Designated by NUCC) 16. CATES ANTENNABLE TO WORK IN CURAPAT SIPATISSY 18. HOSPITALIZATION DATES RELATED TO CURRENT SERVICES " TROU 20. OUTSDE LAS VES 22. ASSION M TO TEGNOSIS OR NATURE OF TELNESS OR INJURY RAL 1 Bervice (24) SCHARGER CD OL GL KL ORIGINAL REF NO H 22. PRIOR AUTHORIZATION NUMBER FIGURE 15 A 312 UNIT THREE CODING AND H POT G OR UNITS DAYS 10 QUAL PROVIDERE JOAGNOSIS PONTER CHAROES 2A DATE OF VICE From To MM DO YY MM DD 1 PROCEDURES, SERVICES, OR SUPPLIES ( harus CPT MORCS1 MOOVER NPI CEO YYSPEMO NPI 2 NPI 3 NPI I 3 4 5 NPI 6 30. Par 25. FEDERAL TAX LD NUMBER SSN EIN 20. PATIENT'S ACCOUNT NO 27. ACCEPTANSIONUENT? YES NO 22. SERVICE FACILITY LOCATION INFORMATION NPI 20 TOTAL CHARGE 29. AMOUNT PAID $ 33. BILLING PROVIDER INFO & PH 31. SIGNATURE OF PHYSICIAN OR SUPPLIER INCLUDING DEGREES OR CREDENTIALS only that the statements on the tilant are made a part of a. NP DONED DATE NPT NUCC Instruction Manual available at: www.nuoc.org PLEASE PRINT OR TYPE APPROVED OMG-098-1197 FORM 1500 101 Chapter 15 Medical Biling and Rembursement Essentials 329 Procedure 15.5 Utilize Medical Necessity Guidelines: Respond to a "Medical Necessity Denied" Claim Name Date Poke to resolve the insurance company's denial of a claim for medical necesity by completing an accurate Score claim Equipment and Supplies . Paper method: Patient's health record, copy of patient's insurance ID card or cards, patient registration form, encounter form, blank CMS-1500 Health Insurance Claim Form (Work Product 15-2), and a pen Electronic method: SimChart for the Medical Office Insurance denial letter or scenario (see below) DOB: 08/07/1944 ICD: G43.101 (Migraine) Scenario: You are working at Walden-Martin Family Medical Clinic, 1234 Anystreet, Anytown, AL 12345 (phone: 123-123-1234). You receive a letter indicating that Medicare has denied the following claim for not being medically necessary: Patient: Norma B. Washington Date of Service: 06/13/20XX Policy/ID Number: 847744144A Provider: Julie Walden MD CPT: 13420 (B-12 injection) You did some research and the information above was the only information sent to Medicare for that encounter. The following information was the correct information for the encounter Patient Norma B. Washington DOB: 08/01/1944 Date of Service: 06/15/20XX ICD: G13.101 (Migraine) CPT: J1885 (Toradol 15 mg-$15.50) and 90772 (Injection, Ther/ Proph/Diag-525.00) ICDD51.0 (Vitamin B, deficiency anemia) CPT: 13420 (B, injection-$24.00) and 90772 (Injection, Ther/Proph/Diag-$25.00) To be billed to: Medicare, 1234 Insurance Road, Anytown, AL 12345-1234 Standard: Complete the procedure and all critical steps in minutes with a minimum score of 85% within two attempts (or as indicated by the instructor). Scoring: Divide the points earned by the total possible points. Failure to perform a critical step, indicated by an asterisk (*), results in grade no higher than an 84% (or as indicated by the instructor), a Time: Began Ended Total minutes Point Value 20 Attempt 1 Attempt 2 Steps: 1 Review the insurance denial letter (scenario) carefully. Compare the patient's information from the denial letter to the health record, claim, and encounter form. Look for errors in the patient's name and date of birth. 2. Compare the insurance denial letter (scenario) to the health record, claim, and encounter form. Look for errors in the date of service, the diagnosis, and the procedure codes. The procedure must be medically necessary for the diagnosis indicated, 20" Copyright 2020. Elsevier Inc. All Rights Reserved 330 Chapter 15 Medical Billing and Reimbursement Essentials 20 insured. 20 3. Complete a claim (either CMS-1500 or an electronic claim using SimChart) by entering in the information about the carrier, patient, and 4. Enter the information regarding the physician, procedures, and diagnosis. Make sure to include all of the information from the encounter. 5. Proofread the claim form for accuracy before submitting the claim. 20 100 Total Points FD HEALTH INSURANCE CLAIM FORM APPROVED BY NATIONAL UN FORM CLAIM COMMITTEE (NUCC) 0012 CARRIER BEROA 1. MEDICARE MEDICAID Dimo (Medicaid #) TRICARE CHAMPUS CHAMPVA PICABIE OTHER Medicare Sponsors SSN member 10 GROUP HEALTH PLAN FECA BLK LUNG (SSN) IND FIGURE 15.2 Section 1 Comer (Block 1). MEDICARE CHAMPVA MEDICAIC TRICARE no PATIENTS NAMEL Name. For me, Motor GROUP HETEN FECA PINO OTHER DUTER For Program in 1 3 PATIENTS BIRTH DATE W DO YY SEX EDIA SATIENTS ADORESSINS 6. PATIENT RELATIONSHIP TO INSURED Sell Soune CH Other STATE B. RESERVED FOR NUCCUSE CITY CITY STATE TELEPHONE (Include Area Code) ZIP COOL TELEPHONE (Include Area Code) OTHER INSURED'S NAME(Last Name First Name, Middle ) 10.IS PATIENTS CONDITION RELATED TO 11.NET OTHER INSURED'S POLICY OR GROUP NUMBER EMPLOYMENT DATE OF SEX WM DO YES NO RESERVED FOR NUOC USE D. AUTO ACCIDENT PLACE(S) OTHER CLAIM YES NO RESERVED FOR NUCC USE OTHER ACCOUNT VES ON SUNCE PLAN NAME OR PROCIRAM NAME 10d. CLAIM CODES (Designated by NUCC) Yes No If yes, cortoms and READ BACK OF FORM BEFORE COMPLETING & SIGNING THIS FORM 13. UNGURED'S OR AUTHORIZED PERSONS SIGNATURE I authorize IR PATIENTS OR AUTHORIZED PERSON'S SIGNATURE I authorize the release of any medical of the information costar payment of medical benefits to the undersigned physician or supplier for services described below is clamo request payment of government benefits other to myself or to the party who accepts diment PATIENT AND INSURED IN DATE SIONID BONEO Islami (wks in tn 13 my and Heimbursement Essentials 311 YY DO QUAL QUAL NOTE O CLIENTETINESS INUIRY, or PREGNANCYILMP16 OTHER DATE EGUE OF REFERRING PROVIDER OR OTHER SOURCE 8 09 178 17 FROM TO MEADOTIONAL CLAIM INFORMATION Designated by NUCC) 16. CATES ANTENNABLE TO WORK IN CURAPAT SIPATISSY 18. HOSPITALIZATION DATES RELATED TO CURRENT SERVICES " TROU 20. OUTSDE LAS VES 22. ASSION M TO TEGNOSIS OR NATURE OF TELNESS OR INJURY RAL 1 Bervice (24) SCHARGER CD OL GL KL ORIGINAL REF NO H 22. PRIOR AUTHORIZATION NUMBER FIGURE 15 A 312 UNIT THREE CODING AND H POT G OR UNITS DAYS 10 QUAL PROVIDERE JOAGNOSIS PONTER CHAROES 2A DATE OF VICE From To MM DO YY MM DD 1 PROCEDURES, SERVICES, OR SUPPLIES ( harus CPT MORCS1 MOOVER NPI CEO YYSPEMO NPI 2 NPI 3 NPI I 3 4 5 NPI 6 30. Par 25. FEDERAL TAX LD NUMBER SSN EIN 20. PATIENT'S ACCOUNT NO 27. ACCEPTANSIONUENT? YES NO 22. SERVICE FACILITY LOCATION INFORMATION NPI 20 TOTAL CHARGE 29. AMOUNT PAID $ 33. BILLING PROVIDER INFO & PH 31. SIGNATURE OF PHYSICIAN OR SUPPLIER INCLUDING DEGREES OR CREDENTIALS only that the statements on the tilant are made a part of a. NP DONED DATE NPT NUCC Instruction Manual available at: www.nuoc.org PLEASE PRINT OR TYPE APPROVED OMG-098-1197 FORM 1500 101