Summarize attached article images COSTS & SPENDING EXHIBIT 2 National health expenditures (NHE) amounts and annual growth, by spending category, calendar years 2012-13 Spending category
Summarize attached article images
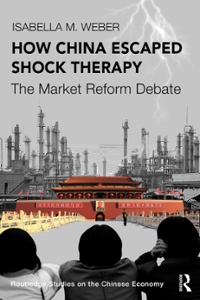
COSTS & SPENDING EXHIBIT 2 National health expenditures (NHE) amounts and annual growth, by spending category, calendar years 2012-13 Spending category expst-rune AMOUNT NHE, billions Health consumption expenditures Personal health care Hospital care Professional services Physician and clinical services Other professional services Dental services Other health, residential, and personal care Home health care Nursing care facilities and continuing care retirement communities Retail outlet sales of medical products Prescription drugs Durable medical equipment Other nondurable medical products Government administration Net cost of health insurance Government public health activities Investment Noncommercial research Structures and equipment ANNUAL snow-m NHE Health consumption expenditures Personal health care Hospital care Professional services Physician and clinical services Other professional services Dental services Other health. residential. and personal care Home health care Nursing care facilities and continuing care retirement communities Retail outlet sales of medical products Prescription drugs Durable medical equipment Other nondurable medical products Government administration Net cost of health insurance Government public health activities Investment Noncommercial research Structures and equipment 2012' 52,791 .1 2.6377 2.361 .1 902.5 743.2 557.1 76.4 109.7 139.1 78.3 1 47.4 350.6 253.0 43.7 53.9 34.2 1 65.2 77.2 1 53.3 48.4 1 05.0 4.0% 4. 1 4. 1 6.0 3.7 4.0 5.0 1 .6 5.6 4.9 1 .4 1 .0 0.4 3.4 2.0 3.9 4.0 3.7 2.8 2.4 5.4 2013 52875.0 2,720.9 2,431.2 937.6 759.6 569.6 78.7 1 1 1 .2 1 44.3 81.4 1 49.0 359.3 258.2 45.1 56.0 37.5 1 73.3 79.0 1 54.1 46.7 1 07.5 3.0% 3.2 3.0 3.9 2.2 2.2 3.0 1.4 3.7 3.9 1.1 2.5 2.1 3.2 3.9 9.6 4.9 2.3 0.5 3.5 2.4 2014 53025.4 2,875.6 2,556.0 978.2 792.5 595.7 83.0 1 13.8 1 51 .5 84.8 1 52.4 396.6 292.4 46.7 57.5 42.3 1 95.3 82.0 1 49.8 2015 2016 2017 2018 53.1 99.6 53347.4 53.4873 53.6494 3,045.5 3,190.7 3,319.0 3,475.0 2,710.2 2,838.3 2,954.5 3,075.5 1,034.6 1,089.5 1,140.6 1.1918 837.9 883.2 924.0 965.1 631.2 665.6 696.9 725.6 87.8 92.7 97.5 103.9 118.8 124.9 129.6 135.6 164.5 173.6 1832 191.6 89.2 93.0 971 102.2 158.1 163.0 1662 168.5 425.9 436.0 4432 456.3 317.1 322.3 326.8 335.0 48.6 51.0 52.4 54.9 60.2 62.7 64.1 66.4- 428 44.9 44.8 47.5 206.7 218.8 228.3 258.5 85.8 88.7 91,4 93.5 154.1 156.7 1683 174.4 46.4 47.4 50,1 52.6 107.7 109.3 1182 121.8 5.8% 4.6% 4.2% 4.6% 5.9 4.8 4,0 4.7 6.0 4.7 4,1 4.1 5.8 5.3 4,7 4.5 5.7 5.4 4,6 4.4 6.0 5.4 4.7 4.1 5.9 5.5 5.2 6.5 4.4 5.1 3.8 4.6 8.6 5.5 5.5 4.6 5.3 4.2 4.5 5.2 3.8 3.1 2,0 1.4 7.4 2.4 1,7 2.9 8.4 1.7 1,4 2.5 4.1 4.9 2.9 4.7 4.7 4.1 2.2 3.6 1.2 5.0 0.2 6.0 5.8 5.9 4.3 13.2 4.6 3.4 3.0 2.4- 2.9 1.7 7,4 3.6 0.8 2.1 5,7 5.0 3.8 1.5 8,1 3.0 sounce Centers for Medicare and Medicaid Services. Office of the Actuary. National Health Statistics Group. NOTES Definitions, sources. and methods for NHE categories can he found in Centers for Medicare and Medicaid Services. National Health Expenditure Accounts: methodology paper (see note 20 in text). Numbers might not add to totals because of rounding. Percent changes are calculated from unrounded data. aAnnual growth. 2011712. Factors Accounting For Growth Exhibit 3 breaks down growth in per capita na- tional health care spending into the factors that account for such growth: the use and intensity of services. medical prices (which reectboth econ- omywide and excess medicalspecific ination) . and the changing age and sex composition of the population. Growth in per capita spending accel- 10 HEALTH AFFAIRS JANUARY 2020 39:1 erated in 2018 to 4.0 percent, following a rate of 3.5 percent in 2017, as faster growth in medical prices more than offset slower growth in the use and intensity of health care goods and services. In 2018 medical price growth accounted for 2.1 percentage points of the 4.0 percent growth in per capita spending (a 53 percent share), while growth in the residual use and intensity of health Do\" unloaded [mm HealtllA'al-s org on March ll zuzii Copyright Plulcci HUPbTl-ie Pcople-to-Pcuplc Heallh Ioimdaiiun. lot in: personal use only. All xlglns reserved Reuse permissions at HealIhAtt'siismg care goods and services accounted for 1.3 per- centage points (a 33 percent share), and the changing age and sex mix of the population ac- counted for 0.6 percentage points (a 14 per- cent share). Medical price growth of 2.1 percent in 2018 was faster than the rate of 1.3 percent in 2017, in part because of faster growth in economywide ination (as measured by the GDP price index) which increased 2.4 percent in 2018 compared to 1.9 percent in 2017 (exhibit 1). Additionally, excess medical-specic price ination beyond economywide price ination declined less in 2018 (0.3percent) than in 2017 (0.6 percent), as faster growth in the net cost of insurance offset some of the negative excess price ination associated with retail prescription drugs and physician and clinical services (data not shown). Although overall medical price growth in 2018 was the most rapid since 2011, the 2018 growth rate of 2.1 percent was below the average annual rate of 3.4 percent during 200407, but the same as the average rate of growth during 200813 (exhibit 3). Residual use and intensity, which reects changes in the use and mix of health care goods and services, grew 1.3 percent in 2018, slower than the rate of 1.6 percent in 2017.5 The services that experienced slower growth in the use and intensity of services in 2018 included hospital care, physician and clinical services, dental ser- vices, home health care, and nursing care facili- ties and continuing care retirement communi- ties. In 2018 the number of uninsured people grew by 1.0 million for the second year in a row to reach 30.7 million (exhibit 4). The increase in the number of uninsured people may have con- tributed to the slowdown in growth in the resid- ual use and intensity of services, as people with- out health insurance may use fewer services.E Sponsors Of Health Care In 2018 the federal government and households accounted for the largest shares of health care spending (28 percent each), followed by private businesses (20 percent), state and local govern- ments (17 percent), and other private revenues (7 percent) (exhibit 5)_ Faster overall spending growth was due to spending from the federal government and private businesses, which expe- rienced faster growth in 2018more than off- setting slower spending growth for state and local governments and other private revenues. For the federal government, spending growth on health care accelerated in 2018 to 5.6 percent, compared to a rate of 2.8 percent in 2017. The acceleration in 2018 was driven mainly by faster growth in the federally sponsored portion of ex- EXHIBIT 3 Factors accounting for gramh in per capita national health expenditures (NHE), selected calendar years 2004-18 6% 5% 4% 7 Residual use 3% 7 andintensity 2% 2 Medical prices 1% - I. I... Age\" 0% 7 sex factors 200407 200813 2014 2015 2016 2017 2018 sounce Centers for Medicare and Medicaid Services, Office of the Actuary, National Health Statis- tics Group. ares Medical price growth, which includes economywide and excess medical-specific price growth (or changes in medical-specific prices in excess of economywide inflation), is calculated using the chain-weighted NHE price deflate-r, \"Residual use and intensity" is calculated by removing the effects of population, age and sex factors. and price growth from the nominal expenditure level. penditures for the Medicare program (a 32 per- cent share), which increased 6.5 percent in 2018 compared to 1.3 percent in 2017 (data not shown). Furthermore, growth in spending on the federal portion of Medicaid payments (a 36 percent share) accelerated to 3.2 percent in 2018 after growth of 0.3 percent in 2017the rst year that states were required to fund 5 per- cent of the spending for the Medicaid expansion population (exhibit 1). In the years before 2017, these costs were funded entirely by the federal government. For state and local governments, spending on health care grew more slowly in 2018, increasing 2.5 percent after a rate of 3.6 percent in 2017 (exhibit 5). The deceleration in 2018 was driven by slower growth in state and local Medicaid spending (which represented 38 percent of total health spending for state and local govern- ments), State and local Medicaid spending grew 2.6 percent in 2018 after growing 6.5 percent in 2017again reecting the increased state fund ing responsibility for the expansion population discussed above (exhibit 1). Household health care spending includes out ofpocket spending, contributions to private health insurance premiums, and contributions to Medicare through payroll taxes and the pay ment of premiums. In 2018 health care spending by households grew 4.4 percentthe same rate JANUARY 2020 11 Manama rm... HealthAffai-s Dlg on March 3: , 2am, Copyright my\": unpem \"spamming mum lawman. Inc. 3921 HEALTH AFFAlRS For personal use only All (isms men/ed Reuse permissions a HeallhAFfairs.plg COSTS 8t SPENDING 12 EXHIIIT 4 National health expendimres (NHE) and health insurance enrollment, aggregate and per enrollee amounts, and annual growth, by source of funds, calendar years 2012-10 2012' 2013 PIIVA'I'E HEALTH INSLIRANCE Expenditure (bi lions) $922.0 $939.1 Expenditure growth 3.5% 1.9% Per enrollee expenditure $4,825 54,916 Per enrollee expenditure growth 1.9% 1.9% Enrollment (mil ions) 191.1 191.0 Enrollment growth 1.7% 0.0% MEDICARE Expenditure (bi lions) $566.5 $588.9 Expenditure growth 4.3% 3.6% Per enrollee expenditure $11,441 $11,485 Per enrollee expenditure growth 0.3% 0.4% Enrollment (mil ions) 49.7 51.3 Enrollment growth 4.1% 3.2% "solemn Expenditure (bi lions) $422.9 $445.2 Expenditure growth 4.0% 5.3% Per enrollee expenditure $7,278 $7,536 Per enrollee expenditure growth 0.6% 3.5% Enrollment (mil ions) 58.1 59.1 Enrollment growth 3.3% 1.7% unmsunen am: popuu'non Uninsured (millions) 44.7 44.1 Uninsured growth 1.9% 1.4% Population (millions)h 313.3 315.5 Population growth 0.7% 0.7% Insured share o1c total population 85.7% 66.0% 2014 2015 2016 2017 2010 5994.1 $1,060.91 511 19.9 $11750 51.2430 5.9% 6.7% 5.6% 4.9% 5.8% 55,106 $5,296 55,550 $5,813 56,199 3.9% 3.7% 4.8% 4.7% 6.7% 194.7 200.3 201 .8 202.1 200.5 1.9% 2.9% 0.7% 0.2% D.8% 5618.5 5648.8 $676.8 $705.1 5750.2 5.0% 4.9% 4.3% 4.2% 6.4% 511,704 511,951 512,137 $12,334 512,784 1.9% 2.1% 1.6% 1.6% 3.7% 52.8 54.3 55.8 57.2 58.7 3.1% 2.7% 2.7% 2.5% 2.6% $497.8 $542.6 $565.4 $580.1 5597.4 1 1.8% 9.0% 4.2% 2.6% 3.0% $7,592 $7,835 $7,948 $8,041 $8,201 0.7% 3.2% 1.4% 1.2% 2.0% 65.6 69.3 71 .1 72.1 72.8 1 1.0% 5.6% 2.7% 1.4% 1.0% 35.5 29.5 28.7 29.7 30.7 19.5% 47.0% 2.8% 3.7% 3.1% 317.9 320.1 322.5 324.6 326.6 0.7% 0.7% 0.8% 0.7% 0.6% 88.8% 90.8% 91 .1 % 90.8% 90.6% sounces Centers for Medicare and Medicaid Services (CMS), Office of the Actuary) National Health Statistics Group;and Department of Commerce, Census Bureau. NOTES Definitions, sources, and methods for NHE categories can be found in Centers for Medicare and Medicaid Services. National Health Expenditure Accounts: methodology paper (see note 20 in text). Numbers might not add to totals because of rounding. Percent changes are calculated from unrounded data. aAnnual growth, 2011712.\"Estimates are explained in exhibit I notes experienced in 2017 (exhibit 5). Out-of-pocket health spending (a 36 percent share) increased 2.8 percent in 2018, faster than the growth rate of 2.2 percent in 2017 (exhibit 1), whereas growth in contributions to employer-sponsored private health insurance premiums (a 27 percent share) slowed from 6.8 percent in 2017 to 3.4 per- cent in 2018 (data not shown). Health care spending by private businesses increased at a faster rate in 2018 (6.2 percent) than in 2017 (4.8 percent) (exhibit 5), and the 2018 growth rate was the fastest since 2003 (data not shown) in spite of a slight drop in the num- ber of people covered by employer-sponsored insurance (exhibit 5). Contributions by private businesses to employer-sponsored private health insurance premiums accounted for the largest share of private businesses' health spend- ing in 2018 (77 percent), with such contributions increasing 7.2 percent in 2018, up from a rate of 5.5 percent in 2017. HEALTH AFFAiRS JANUARY 2020 39:1 Private Health Insurance Private health insurance expenditures ac- counted for 34 percent of total national health care spending in 2018 and reached $1.2 trillion (exhibit 1). Spending in this category increased 5.8 percent in 2018, which was a faster rate than the 4.9 percent growth experienced in 2017. Private health insurance spending for medical goods and services grew 4.5 percent in 2018, similar to the growth rate of 4.3 percent in 2017, while the net cost of private health insur- ance (which represents 64 percent of the total net cost of health insurance) increased rapidly in both years9.5 percent in 2017 and 15.3 percent in 2018 (data not shown). The 4.5 percent growth in medical goods and services paid for by private health insurance re- ected mixed trends in underlying goods and services, as spending for hospital care' retail prescription drugs, dental services, and other professional services grew more rapidly in 2018 Downloaded from Heaiilmaus mg on Mmis 31.2021) capynm mm HOPbiTlie PeoplerlorFeople Health roundallun. inc. m permmi use only All \"gum resolved amt-e pennisiions at minimum org EXHIBIT 5 National health expenditures (NHE) amounts, annual growth, and percent distrilmtion. by type of sponsor, calendar years 2012-18 Type of sponsor 2012' 2013 2014 2015 2016 2017 2018 sxrsunlruns AMOUNT NHE. billions 52791.1 52.8750 53.0254 53199.6 33347.4 53487.3 53649.4 Businesses, household, and other private revenues 1,572.2 1,6153 1,666.1 1,742.6 1,828.0 1,921.0 2,013.1 Private businesses 564.9 573.6 599.0 622.7 652.8 684.2 726.8 Household 807.7 834.4 862.5 908.1 950.5 992.5 1,035.7 Other private revenues 199.5 2073 204.6 21 1.7 224.7 244.3 250.7 Governments 1.2189 1,259.8 1.3592 1,457.0 1.5194 1,566.3 1,636.3 Federal government 731.3 751.9 835.1 908.1 951.9 978.5 1,033.8 State and local governments 487.6 507.9 524.2 548.9 567.5 587.8 602.5 ANNUAL Guam-M NHE 4.0% 3.0% 5.2% 5.8% 4.6% 4.2% 4.6% Businesses, household. and other private revenues 5.3 2.7 3.1 4.6 4.9 5.1 4.8 Private businesses 4.5 1 .5 4.4 4.0 4.8 4.8 6.2 Household 4.4 3.3 3.4 5.3 4.7 4.4 4.4 Other private revenues 11.5 3.9 1.3 3.5 6.1 8.7 2.6 Governments 2.5 3.4 7.9 7.2 4.3 3.1 45 Federal government 0.2 2.8 1 1.1 8.7 4.8 2.8 5.6 State and local governments 6.1 4.2 3.2 4.7 3.4 3.6 2,5 Pencsur DISTIIBUTION NHE 100% 100% 100% 100% 100% 100% 100% Businesses, household, and other private revenues 56 56 55 54 55 55 55 Private businesses 20 20 20 19 20 20 20 Household 29 29 29 28 28 28 28 Other private revenues 7 7 7 7 7 7 7 Governments 44 44 45 46 45 45 45 Federal government 26 26 28 28 28 28 28 State and local governments 17 18 17 17 17 17 17 sou-cs Centers for Medicare and Medicaid Services. Office of the Actuary, National Health Statistics Group. Il'I'ES Definitions, sources, and methods for NHE categories can be found in Centers for Medicare and Medicaid Services. National Health Expenditure Accounts; methodology paper (see note 20 in text). Numbers might not add to totals because of rounding. Percent changes are calculated from unrounded data aAnnual growth, 201 1712, while spending growth for physician and clinical services, nursing home care, home health care, and durable medical equipment decelerated. The net cost of private health insurance reached $164.3 billion and grew 15.3 percent in 2018, its fastest rate of increase since the 2003 increase of20.7 percent (data not shown).7 The faster growth in the net cost was driven in large part by the reinstatement of the health insurance tax in 2018, following a one-year mor- atorium in 2017.8 Private health insurance enrollment declined slightly (0.8 percent) in 2018, prinlarily be- cause of declines in enrollment in other directly purchased plans (non-Marketplace plans) and employer-sponsored insurance plans (exhibit 4). Enrollment in other directly purchased plans declined by 1.4 million people, as average pre- miums increased}lU For employer-sponsored private health insurance coverage, enrollment declined 0.2 percent, as data indicate that em- ployees took up offers of insurance at a slightly lower rate in 2018.ll Per enrollee, spending for private health insurance was $6,199, an increase of 6.7 percent over 2017. This is the highest per enrollee spending growth rate since the 2004 growth rate of 7.5 percent but similar to the growth rate of 6.6 percent in 2009, when per- sonal health care spending was the main driver. In 2018 the net cost of private health insurance was the signicant factor behind the rapid growth (data not shown). Medicare Medicare spending represented 21 percent of all national health care spending in 2018 and reached $750.2 billion (exhibit 1). Total Medi- care spending growth accelerated in 2018 to 6.4 percent, compared to a rate of 4.2 percent in 2017. Medicare enrollment growth was fairly steady, accelerating 0.1 percentage point to 2.6 percent (exhibit 4) . Accordingly, per enrollee Medicare expenditures grew more rapidly in JANUARY 2020 39:1 Downloaded from HealthAlen org on March 3 l, 201" Copyright Project HOPE/711m Pcuplcrtorl'eoplc Health toundaomi. Inc, impersonal use only All rights rescued Reuse Permlssiutls at Healile'nln; org HEALTH AFFAIRS l3 COSTS & SPENDING 14 2018, increasing 3.7 percent from a growth rate of 1.6 percent in 2017. The low per enrollee ex- penditures in 2017 reected slow growth in Medicare private plan spending resulting from the suspension of the health insurance tax. Medicare spending on nonpersonal health care, which includes government administration and the net cost of insurance for Medicare pri- vate health plans, was one of the drivers of faster growth in the program in 2018.12 Growth in non personal health care spending rose from a de- cline of 2.4 percent in 2017 to an increase of 16.0 percent in 2018, largely as a result offaster growth in the net cost of insurance as private Part C and Part D plans adjusted their premiums to reect the expiration of the moratorium on the health insurance tax (data not shown). In addition, growth in Medicare government ad- ministrative expenditures rebounded from a de- cline in 2017 to positive growth in 2018, contrib- uting to the acceleration in Medicare non personal health care spending in 2018. The de- cline in Medicare administrative expenditures in 2017 was largely attributable to the impact of recoveries for excess Medicare administrative expenses that had been paid by the federal gov- ernment prospectively in prior years. These re- coveries more than offset government adminis- trative costs that had been disbursed during 2017. In contrast, Medicare personal health care spending accelerated just one percentage point. from a rate of4.7percent in 2017 to 5.7 percent in 2018, as spending growth for most goods and services accelerated in 2018. Feeforservice Medicare spending accounted for 64 percent of overall Medicare spending in 2018, down slightly from a 66 percent share in 2017 as a result of slower growth in fee-for- service enrollment compared to Medicare Ad- vantage enrollment. In 2018 spending in fee- forservice Medicare grew 3.5 percent, after a smaller increase of 1.4 percent in 2017. In both 2017 and 2018 fee-for-service Medicare enroll- ment remained steady at thirty-eight million people, accounting for 65 percent of total Medi- care enrollment in 2018. Growth in per enrollee fee-for-service Medicare expenditures accelerat- ed from 1.5 percent in 2017 to 3.6 percent in 2018. This faster growth was inuenced by faster per enrollee expenditure growth for physician and clinical serviceswhich was attributable, in turn, to an increase in the volume and inten- sity of services and an acceleration in spending growth for physician-administered drugs. Addi- tionally, faster growth in Medicare spending for durable medical equipment resulted from an in- crease in the volume and mix of products con- sumed, following numerous years of declines associated with the implementation of competi- HEALTH AFFAIRS JANUARY 2020 39:1 tive bidding for these products. Medicare private health plan spending (the majority of which is associated with Medicare Advantage plans) increased 11.8 percent in 2018, faster than the rate of 9.9 percent in 2017. En- rollment in Medicare private health plans in- creased 7.9 percent in 2018, about the same rate as in 2017. Continued faster enrollment growth in these plans, compared to fee-for-service Medi- care, increased the share of enrollment in private plans to 35 percent of total Medicare enrollment in 2018. At the same time, Medicare private health plans also continued to account for a larg- er portion of total Medicare spending, at 36 per- cent in 2018a 6-percentage-point increase since 2014. Per enrollee spending for Medicare private health plans grew 3.6 percent, which was faster than per enrollee growth of 1.7 percent in 2017 mostly because of faster growth in the net cost of insurance for private plans that resulted from the reinstatement of the collection of the health insurance tax. Medicaid Medicaid spending by federal and state and local governments accounted for 16 percent of nation- al health care spending and reached $597.4 bil- lion in 2018 (exhibit 1). Medicaid spending in- creased 3.0 percent in 2018 after growing 2.6 percent in 2017. The faster growth in 2018, which was inuenced by the net cost of insur- ance, was partly offset by a deceleration in en- rollment growth and slower spending growth for Medicaid managed care goods and services. Medicaid enrollment growth most recently peaked in 2014, when numerous states expand- ed eligibility to certain adults, but growth slowed each year thereafter (exhibit 4). Medicaid enroll- ment is estimated to have increased 1.4 percent in 2017 and 1.0 percent in 2018. The slower growth in Medicaid enrollment in 2018 was largely the result of stronger economic growth.13 Medicaid per enrollee spending growth acceler- ated to 2.0 percent in 2018 from 1.2 percent in 2017, primarily because of the increased growth in the net cost of insurancewhich was driven both by the decrease in recovery payments from Medicaid managed care plans to the federal gov- ernment and by the health insurance tax.\" Medicaid hospital spending, which accounted for a third of total Medicaid spending, increased 2.0 percent in 2018 compared to 1.9 percent in 2017 (data not shown), as a slowdown in growth in Medicaid managed care payments was more than offset by faster growth in Medicaid supple- mental payments to hospitals.15 The second and third-largest Medicaid servicesother health, residential, and personal health care services unwnloadm [mm HCiulAalr) or; an March 31 Join. Copyright Fromm "OFF n).- Peuyiermrl'cupie malm laundaliun. Inc. in. pcmmi m only An nglln micncd muse permissions at HcailliAtlhuiurg and physician and clinical servicesboth expe- rienced slower spending growth in 2018, at rates of 4.9 percent (down from 6.0 percent in 2017) and 2.9 percent (down from 4.2 percent in 2017), respectively. For Medicaid other health, residen- tial, and personal care services, the slower growth in spending in 2018 resulted partly from slower growth in nonwaiver services, such as school-based and rehabilitative services. For Medicaid physician and clinical services, the de- celeration in spending growth reected slower growth in Medicaid managed care payments for physician and clinical services as well as slower growth in fee-for-service payments to clinics. Medicaid state and local spending grew 2.6 percent in 2018, a slower rate than the rate of 6.5 percent in 2017 (exhibit 1). The fastergrowth in 2017 was largely attributable to the initial requirement that states fund 5 percent of the costs for the expansion population. Federal spending grewslightly faster than state and local spending, increasing 3.2 percent in 2018 after growing only 0.3 percent in 2017. States that expanded Medicaid to eligible adults were re- quired to fund 6 percent of the costs for this population in 2018, up one percentage point from the 5 percent rate in 2017. Hospital Care Hospital care spending increased at about the same rate in both 2017 and 2018 (4.7 percent and 4.5 percent, respectively) to reach $1.2 tril- lion in 2018, or 33 percent of total health care spending (exhibit 2). Hospital prices increased 2.4 percent in 2018 compared to 1.7 percent in 2017, while nonprice factors (such as the use and intensityofservices) grew more slowlyin 2018.15 Growth in total inpatient days was slower in 2018 at 0.7 percent, after 1.7 percent growth in 2017.17 Hospital care was paid for largely by private health insurance, Medicare, and Medicaid, which together accounted for over three-quar- ters of all hospital expenditures in 2018. Spend- ing for hospital care by private health insurance (a 40 percent share) increased at 5.9 percent, and such spending by Medicare (a 25 percent share) increased at 4.6 percentifaster than in 2017while Medicaid hospital spending growth remained around 2 percent (data not shown). Slower growth in other private hospital revenue and out-of-pocket spending forhospital services, combined with a decline in spending from the Department of Defense, more than offset the faster growth in private health insurance and Medicare spending for hospital services in 2018. Physician And Clinical Services Spending for physician and clinical services in- creased 4.1 percent in 2018, reaching $725.6 bil- lion or 20 percent of total health care expendi- tures (exhibit 2). This increase followed faster growth of 4.7 percent in 2017, and spending growth slowed for the third consecutive year. Nonprice factors such as the use and intensity of services contributed to the slowdown, while prices for physician and clinical services in- creased 0.7 percent after growing 0.4 percent in 2017.18 While growth in spending for clinical services (6.0 percent) continued to outpace such growth for physician services (3.6 percent) in 2018, each experienced slower growth than in 2017. Spending growth for physician and clinical services was driven by slower growth in spending by private health insurance, Medicaid, and other private revenues. For private health insurance spending, which accounted for 43 percent of total physician and clinical expenditures, growth slowed in 2018 to a rate of3.9 percent, compared to an increase of 4.6 percent in 2017 (data not shown). For Medicaid (an 11 percent share), ex penditure growth also slowed in 2018, increas ing 2.9 percent compared to 4.2 percent in 2017. Furthermore, other private revenues (which includes philanthropy and other nonpatient care income) declined 3.2 percent in 2018, fol- lowing much larger average annual growth of 11.4 percent during 201517. Medicare spending (a 23 percent share) partially offset the overall slowdown in spending growth for physician and clinical services. It accelerated to 7.8 percent in 2018 from 5.9 percent in 2017, primarily because of an increase in the volume and intensity of services and an acceleration in spending growth for physician-administered drugs.19 Retail Prescription Drugs Spending on retail prescription drugs increased 2.5 percent in 2018 to $335.0 billion, and the share of national health spending for this cate gory ofgoods and services remained unchanged at 9 percent (exhibit 2).\" The 2.5 percent in crease in prescription drug spending in 2018 was faster than the 1.4 percent increase in 2017, as increased spending on new oncology and auto- immune drugs was partially offset by a decline in price growth and the continued increase in the use of generic drugs.21 In 2018 faster growth in nonprice factors helped drive the increase in total retail prescrip- tion drug spending growth, while price growth for both generic and brand-name drugs slowed. The number of prescriptions dispensed (based on thirty days' supply) increased 2.7 percent, JANUARY 2020 39:1 Dawnloadad frum HealltlAffairs.urg an Marc]: M 20m. Copyright Projeu Hopeat- hupicmveuple Hmlm Ionmiamn, m, inrpemml use only All ngl: reserved Rum) pennunonj at HeallllAlthii.Dtg HEALTH AFFAIRS 15
Step by Step Solution
There are 3 Steps involved in it
Step: 1
Get Instant Access to Expert-Tailored Solutions
See step-by-step solutions with expert insights and AI powered tools for academic success
Step: 2
Step: 3
Ace Your Homework with AI
Get the answers you need in no time with our AI-driven, step-by-step assistance