

Answered step by step
Verified Expert Solution
Question
1 Approved Answer
Summarize below attachments from article VIEWPOINT Aaron Glickman, BA Department of Medical Ethics and Health Policy, Perelman School of Medicine, University of Pennsylvania, Philadelphia. Sarah

Summarize below attachments from article

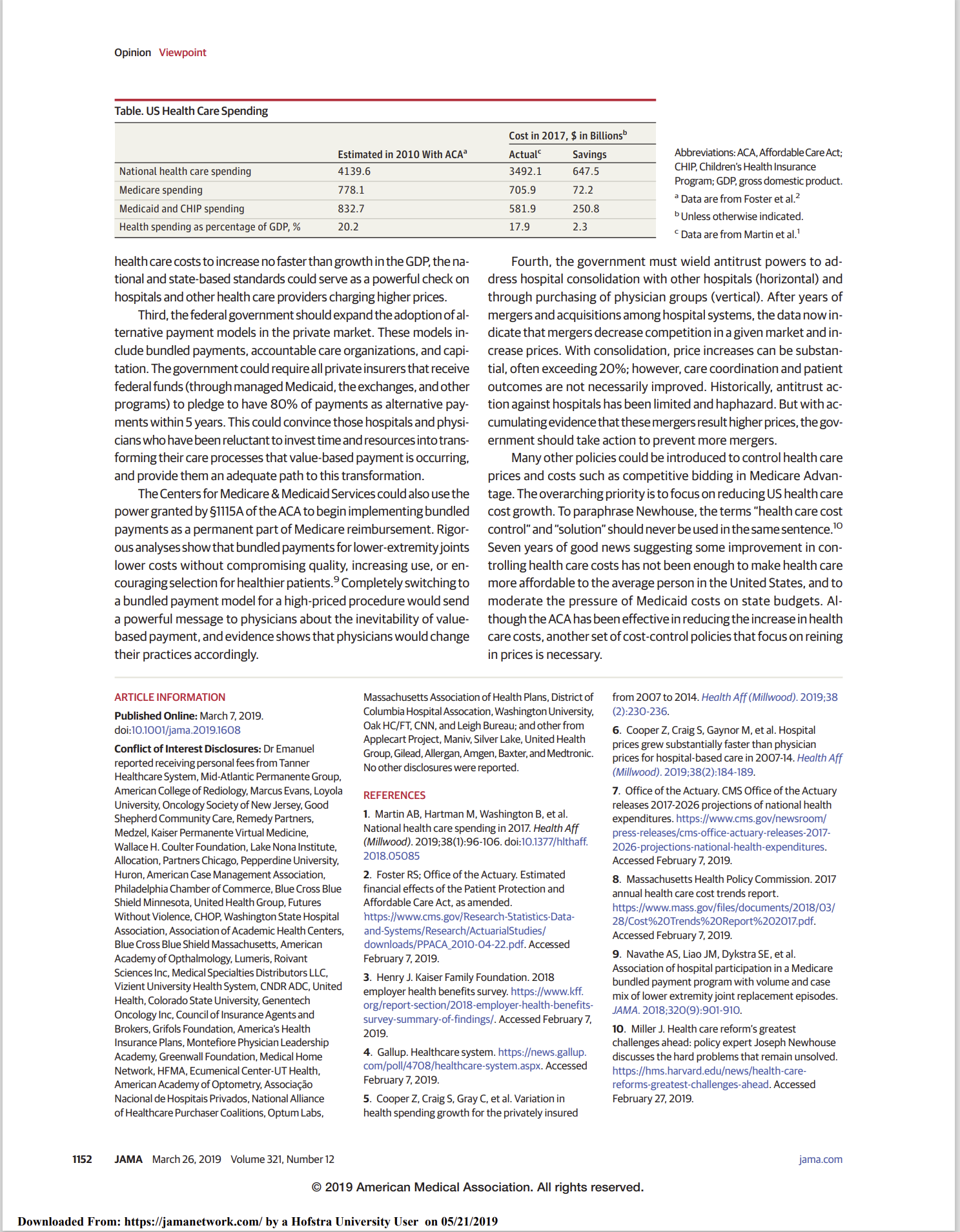
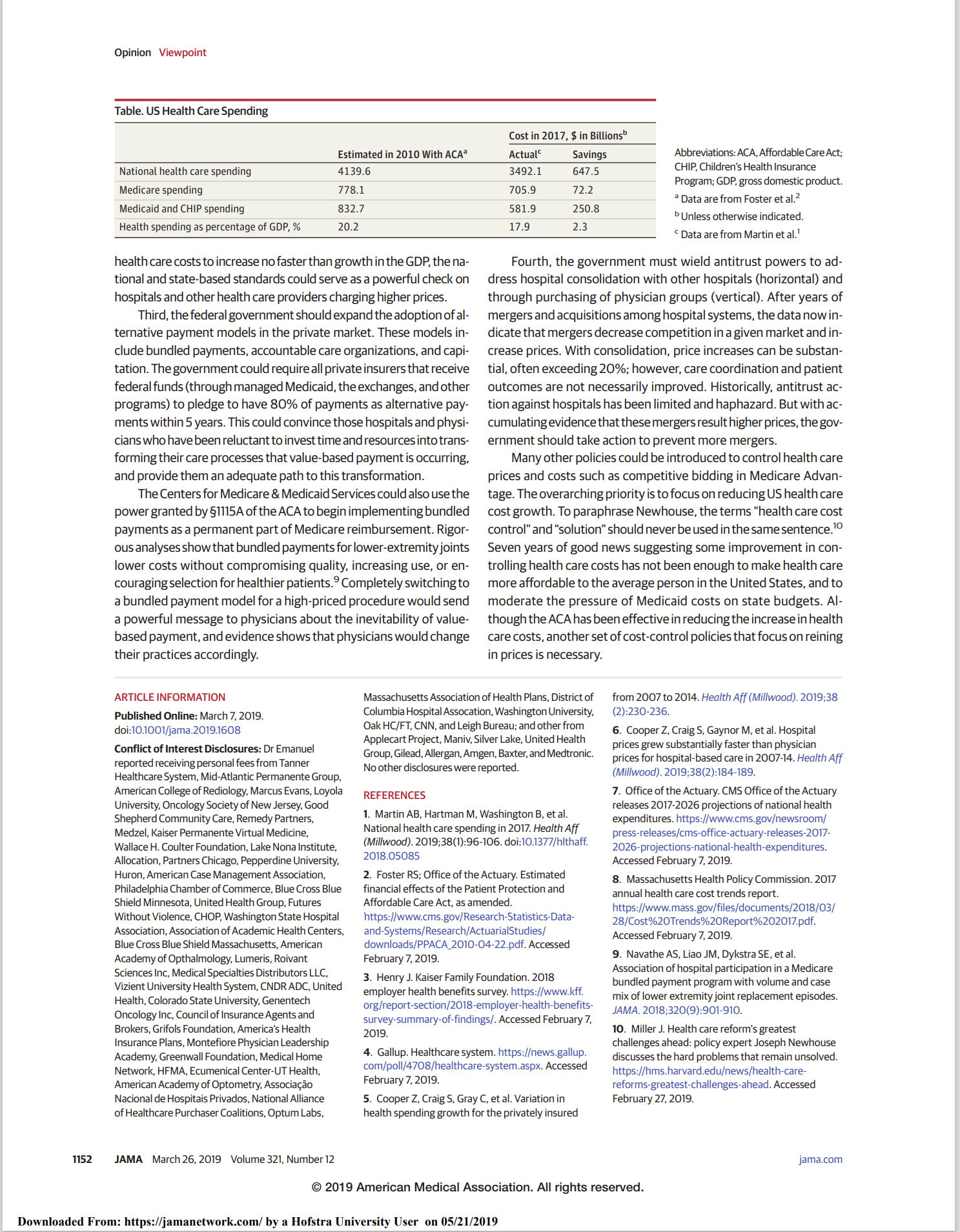
VIEWPOINT Aaron Glickman, BA Department of Medical Ethics and Health Policy, Perelman School of Medicine, University of Pennsylvania, Philadelphia. Sarah S. P. DiMagno, BA Department of Medical Ethics and Health Policy, Perelman School of Medicine, University of Pennsylvania, Philadelphia. Ezekiel J. Emanuel, MD. PhD Department of Medical Ethics and Health Policy, Perelman School of Medicine, University of Pennsylvania, Philadelphia; and Department of Health Care Management, Wharton School, University of Pennsylvania, Philadelphia. Author Audio Interview Corresponding Author: Ezekiel J. Emanuel, MD, PhD, Perelman School of Medicine, University of Pennsylvania, 423 Guardian Dr, Blockiey Hall, ste 1412, Philadelphia, PA 19104 (mehpchair@upenn. edu). Jama.com Opinion Next Phase in Effective Cost Control in Health Care Health care spending is a combination of use and There is some good news on cost control in the United prices. The 2018 Office of the Actuary report2 suggests States. In 2017, the last year for which data are avail- able, health care expenditures were 17.9% of gross do- that health care use is moderating, but a real problem is mestic product (GDP). 1 This is similar to the 2010 level continued price increases.l From 2007 to 2014, (1) pri- of 17.3% when the Affordable Care Act (ACA) was signed vate insurance prices for hospital inpatient services in- into law. On April 22, 2010, one month after enactment creased by 42% and outpatient services increased by of the ACA, the US Department of Health and Human 25% and (2) prices for physician services increased by Services' (DHHS) Office ofthe Actuary released a report.2 6 18% for inpatient care and by 6% for outpatient care. Actual spending has been much better than the official Retail prescription drug spending increased by 12.4% in 2014, 8.9% in 2015, and 2.3% in 2016. I Those spending estimates from the Office of the Actuary (Table). In 2017, total health care costs were almost $650 bil- increases do not even include the rapidly increasing por- lion less than anticipated (Table). Expenditures for Medi- tion of drug spending for Part B specialty drugs for can- care were $72 billion less than the projections and cer, rheumatoid arthritis, and multiple sclerosis. Collec- tively, the rapid increases in prices for drugs and hospital Medicaid and the Children's Health Insurance Program (CHIP) were $250 billion less than the projections. Some services in the private market suggest 4 specific recom- of the Medicaid and CHIP savings may be because not mendations for the next phase of cost-control efforts. all states expanded Medicaid under the ACA; however, First, the United States needs to do more about con- that is a small fraction of the $250 billion. In recent years, trolling drug prices. Spending for drugs accounts for nearly 17% of national health expenditures (inpatient, outpatient, government reports indicate that "overall healthcare spending growth slowed." 1 Importantly, this slowdown and retail), and the future portends ever-increasing drug of cost growth and total spending occurred while insur- prices. Between 2012 and 2017, the proportion of total Medicare spending that went toward paying for drugs in- ance coverage increased to include an additional 20 mil- creased from 17% to 23%.7 The Office ofthe Actuary proj- lion individuals in the United States through the ex- changes, Medicaid expansion, protecting patients with ects annualized increases by 6.3% in drug spending until 2026, which is higher than projections for increases in hos- preexisting conditions, and allowingchildren stay on their pital or physician costs.8 The United States needs national parents' health plan, among other mechanisms. drug price negotiation, not just for Medicare. It should There is also troubling news. In 2017, the per-capita health care spending in the United States was $10 739, cover all US residents and be pegged to standards ofvalue- based pricing and social affordability. Such legislation about 27% more than Switzerland, which is the country looked impossible just a few years ago, but a bipartisan with the next most expensive health care expenditures. The average family premium for employer-sponsored agreement is beginning to emerge. Fully 92% of Repub- health insurance was $19 616 in 2018, representing al- lican voters, along with President Trump and Freedom Cau- most one-third of the median household income of cus members, endorse the need for drug price legislation. $61 372.3 Employees are paying more ofthat cost than ever Second, the secretary of the DHHS should set na- beca use employers are shifting more of the premiums onto tional and state-level benchmarks for total health care cost workers and increasingly adopting high-deductible plans. growth that are linked to economic growth and popula- Simultaneously, prices for specialty drugs are increasing tion aging. Even voluntary cost growth limits can be ef- substantially, with the cost for some drugs and gene and fective in curbing cost growth. In 2012, Massachusetts cellular therapies exceeding $300 000 per course oftreat- established the Health Policy Commission, which moni- ment. In 2019, new gene therapy treatments may sur- tors spending and establishes benchmark limits on health pass $2 million per patient. According to a 2018 Gallup poll care cost inflation based on state GDP growth. The com- mission has limited enforcement resources. Its main that included more than 1000 respondents, people in the power is to identify institutions that contribute to cost United States believe that cost is "the most urgent health problem facing this country at the present time. growth and make this information publicly available. This approach has been successful in that Massachusetts has Even though the United States is doing better on con- trolling cost growth, the extremely high costs of health had 7 years of below-average growth in health care costs, care remain a significant financial and emotional strain. and commercial health care spending has declined by nearly $6 billion between 2012 and 2016.9 Although national trends suggest a significant slowdown in cost growth, those gains are not evenly distributed. Be- Rhode Island, Vermont, and most recently Delaware tween 2007 and 2014, Medicare spending decreased by have adopted the Massachusetts approach. Admittedly this approach may have been effective in Massachusetts 1.2% per capita, whereas spending in private insurance increased by 16.9% per capita.5 Consequently, the fed- because the state has among the highest health care costs eral treasury may be feeling some financial relief, whereas in the country, but the same can be said of the United States compared with the rest of the world. If the secre- many individuals in the employer-based and individual insurance markets are feeling financial pain. tary of the DHHS issued annual benchmarks that allowed JAMA March 26, 2019 Volume 321, Number 12 0 2019 American Medical Association. All rights reserved. 1151 Downloaded From: https://jamanetwork.com/ by a Hofstra University User on 05/21/2019
Step by Step Solution
There are 3 Steps involved in it
Step: 1

Get Instant Access to Expert-Tailored Solutions
See step-by-step solutions with expert insights and AI powered tools for academic success
Step: 2

Step: 3
Ace Your Homework with AI
Get the answers you need in no time with our AI-driven, step-by-step assistance
Get Started
Foundations of Business
Authors: William M. Pride, Robert J. Hughes, Jack R. Kapoor
6th edition
1337386928, 9781337670975 , 978-1337386920