

Answered step by step
Verified Expert Solution
Question
1 Approved Answer
This form below will be a Entity Lab Results This form below will be a Entity Imaging Results This is database question i gave two
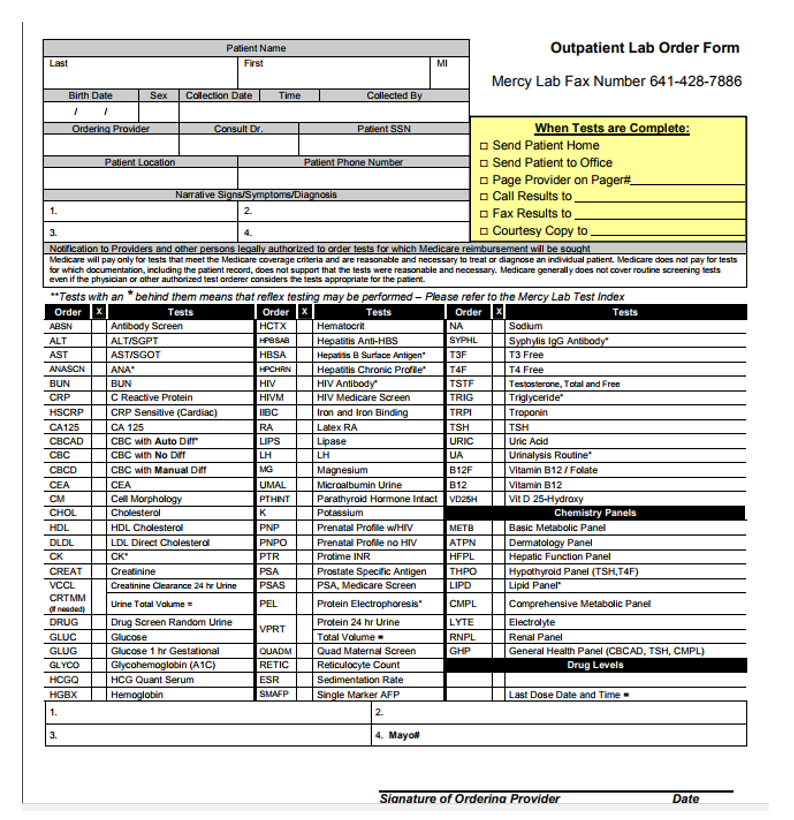
This form below will be a Entity Lab Results
This form below will be a Entity Imaging Results
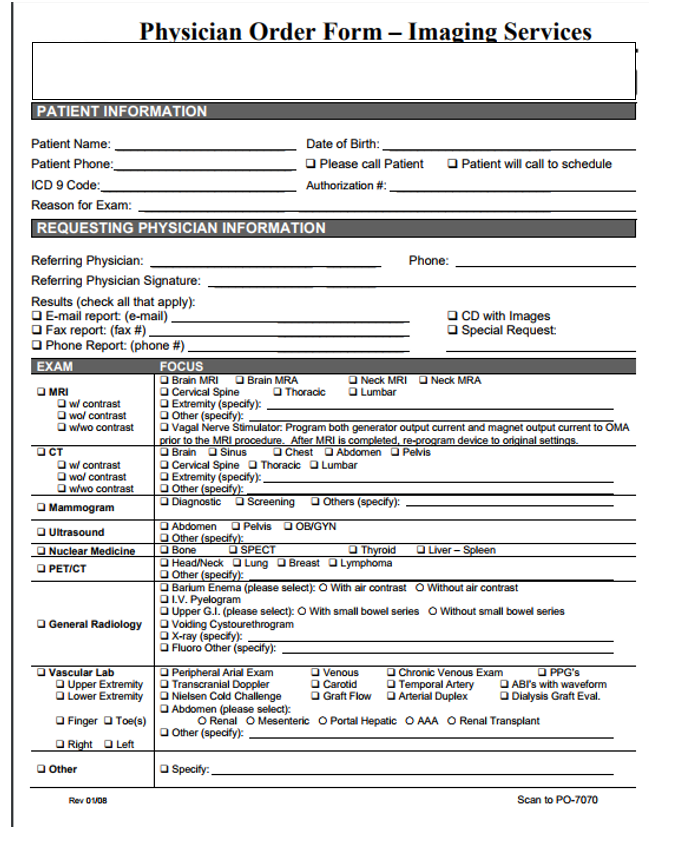
This is database question i gave two forms above and above each form is an entity and i gave u the name of the entity for each form.
So what I need to know is for each form above what would u make the entities attributes and what would you consider candidate keys like primary key or foreign key
so u have the entity are LabResults and ImagingResults
i need attributes for each form above and possible candidate for primary and foreign key
Patient Name Outpatient Lab Order Form MI Mercy Lab Fax Number 641-428-7886 i1 ex Colection DateTim When Tests are Complete: Send Patient Home Send Patient to Office Page Provider on Page Call Results to Fax Results to 3. o Courtesy Copy to Medicare will pay only for tests that meet the Medicare coverage criteria and are reasonable and necessary to treat or diagnose an individual patient. Medicare does not pay for tests for which documentation, inclucing the patient record, does not support that the lests were reasonable and necessary. Medicare generally does not cover routine screening tests even if the physician or other authorized test orderer considers the tests appropriate for the paient Tests with an "behind them means that reflex testing may be perfarmed- Please refer to the Mercy Lab Test Index Antibody Screen ALTISGPT ASTISGOT T3 Free T4 Free Testosterone, Total and Free Triglyceride AST Hepais 8 Surface Antigen* HIV Medicare Screen Iron and Iron Binding Latex RA CRP Sensitive (Cardiac) CA125 CBC with No Diff CBC with Manual Dt CEA Cell Morphology LH LH Urinalysis Routine" itamin B12/Folate Vitamin B12 Vit D 25-Hydroxy CEA Microalbumin Urine PTHINTParathyroid Hormone Intact VD25H Chemistry Panels HDL HDL Cholesterol Prenatal Profile WHIM Prenatal Profile no HIV Basic Metabolic Panel LDL Direct Cholestera ATPN Dermatologv Panel CK CREAT VCCL CRT Creatinine .stain74vneur 2ett E' URawn Urne Total volume Drug Screen Random Urine PSA B PSA, Medicare Screen Lipid Panel Comprehensive Metabolic Panel Protein 24 hr Urine Total Valume. Renal Panel General Health Panel (CBCAD, TSH, CMPL) Glucose 1 hr Gestational Glycohemoglobin (A1C) HCG Quant Serum llt; lli kudleFaibi @3a Sedimentation Rate Drug Levels HGBXHemoglobin Last Dose Date and Time 2. Mayo# Sianature of Orderina Provider Physi ician Order Form -Ima ging Services PATIENT INFORMATION Date of Birth: Please call Patient Patient will call to schedule Authorization # REQUESTING PHYSICIAN INFORMATION Phone Referring Physician Signature Results (check all that apply) D E-mail report (e-mail) O Fax report: (fax #) O CD with Images Special Request Phone Report: (phone #) EXAM FOCUS Brain MRI Brain MRA Neck MRI Neck MRA MRI Cervical Spine Thoracic Lumbar wol contrast who contrast O Other (specify) | O Vagal Nerve Stimulator. Program both generator output current and magnet output current to OMA to the MRI Cervical Spine Diagnostic Brain O Sinus ChestAbdomen Pelvis Thoracic Lumbar wol contrast w/wo contrast Other O Extremity (specify) Screening O Others (specify): Mammogram Abdomen O Pelvis OB/GYN Ultrasound Other Bone Liver PETICT Other Barium Enema (please select): O With air contrast O Without air contrast Upper G.I. (please select: O With small bowel series O Without small bowel series O X-ray (specfy): General Radiology Volding Cystourethrogram Fluoro Other (specify): Vascular Lab Chronic Venous Exam OPPG'S ABrs with waveform Dialysis Graft Eval. Peripheral Arial Exam Upper ExtremityTranscranial Doppler Carotid O Graft Flow O Temporal Artery Lower Extremity | O Nielsen Cold Challenge O Finger OToe(s) O R Arterial Duplex OAbdomen (please select) O Renal O Mesenteric O Portal Hepatic OAAA ORenal Transplant Other (specify): Left Other Specify Rev 0UDB Scan to PO-7070 Patient Name Outpatient Lab Order Form MI Mercy Lab Fax Number 641-428-7886 i1 ex Colection DateTim When Tests are Complete: Send Patient Home Send Patient to Office Page Provider on Page Call Results to Fax Results to 3. o Courtesy Copy to Medicare will pay only for tests that meet the Medicare coverage criteria and are reasonable and necessary to treat or diagnose an individual patient. Medicare does not pay for tests for which documentation, inclucing the patient record, does not support that the lests were reasonable and necessary. Medicare generally does not cover routine screening tests even if the physician or other authorized test orderer considers the tests appropriate for the paient Tests with an "behind them means that reflex testing may be perfarmed- Please refer to the Mercy Lab Test Index Antibody Screen ALTISGPT ASTISGOT T3 Free T4 Free Testosterone, Total and Free Triglyceride AST Hepais 8 Surface Antigen* HIV Medicare Screen Iron and Iron Binding Latex RA CRP Sensitive (Cardiac) CA125 CBC with No Diff CBC with Manual Dt CEA Cell Morphology LH LH Urinalysis Routine" itamin B12/Folate Vitamin B12 Vit D 25-Hydroxy CEA Microalbumin Urine PTHINTParathyroid Hormone Intact VD25H Chemistry Panels HDL HDL Cholesterol Prenatal Profile WHIM Prenatal Profile no HIV Basic Metabolic Panel LDL Direct Cholestera ATPN Dermatologv Panel CK CREAT VCCL CRT Creatinine .stain74vneur 2ett E' URawn Urne Total volume Drug Screen Random Urine PSA B PSA, Medicare Screen Lipid Panel Comprehensive Metabolic Panel Protein 24 hr Urine Total Valume. Renal Panel General Health Panel (CBCAD, TSH, CMPL) Glucose 1 hr Gestational Glycohemoglobin (A1C) HCG Quant Serum llt; lli kudleFaibi @3a Sedimentation Rate Drug Levels HGBXHemoglobin Last Dose Date and Time 2. Mayo# Sianature of Orderina Provider Physi ician Order Form -Ima ging Services PATIENT INFORMATION Date of Birth: Please call Patient Patient will call to schedule Authorization # REQUESTING PHYSICIAN INFORMATION Phone Referring Physician Signature Results (check all that apply) D E-mail report (e-mail) O Fax report: (fax #) O CD with Images Special Request Phone Report: (phone #) EXAM FOCUS Brain MRI Brain MRA Neck MRI Neck MRA MRI Cervical Spine Thoracic Lumbar wol contrast who contrast O Other (specify) | O Vagal Nerve Stimulator. Program both generator output current and magnet output current to OMA to the MRI Cervical Spine Diagnostic Brain O Sinus ChestAbdomen Pelvis Thoracic Lumbar wol contrast w/wo contrast Other O Extremity (specify) Screening O Others (specify): Mammogram Abdomen O Pelvis OB/GYN Ultrasound Other Bone Liver PETICT Other Barium Enema (please select): O With air contrast O Without air contrast Upper G.I. (please select: O With small bowel series O Without small bowel series O X-ray (specfy): General Radiology Volding Cystourethrogram Fluoro Other (specify): Vascular Lab Chronic Venous Exam OPPG'S ABrs with waveform Dialysis Graft Eval. Peripheral Arial Exam Upper ExtremityTranscranial Doppler Carotid O Graft Flow O Temporal Artery Lower Extremity | O Nielsen Cold Challenge O Finger OToe(s) O R Arterial Duplex OAbdomen (please select) O Renal O Mesenteric O Portal Hepatic OAAA ORenal Transplant Other (specify): Left Other Specify Rev 0UDB Scan to PO-7070Step by Step Solution
There are 3 Steps involved in it
Step: 1

Get Instant Access to Expert-Tailored Solutions
See step-by-step solutions with expert insights and AI powered tools for academic success
Step: 2

Step: 3
Ace Your Homework with AI
Get the answers you need in no time with our AI-driven, step-by-step assistance
Get Started