

Answered step by step
Verified Expert Solution
Question
1 Approved Answer
she 4. How should Dr. Lopez translate her budget into a capitation rate that can propose to Continental? What other issues should she consider
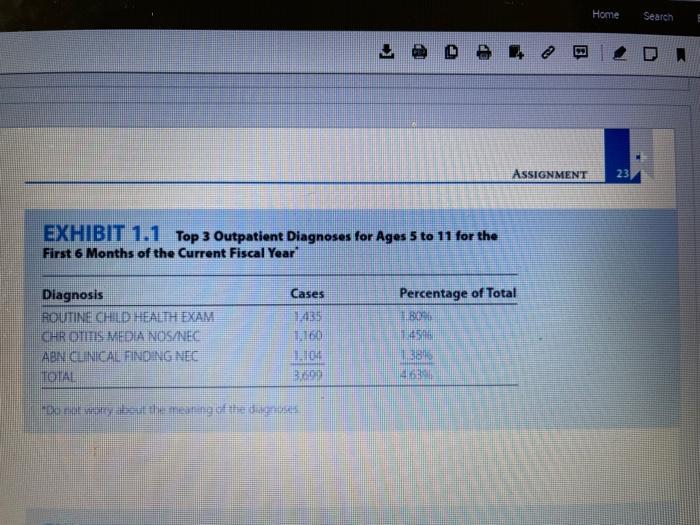
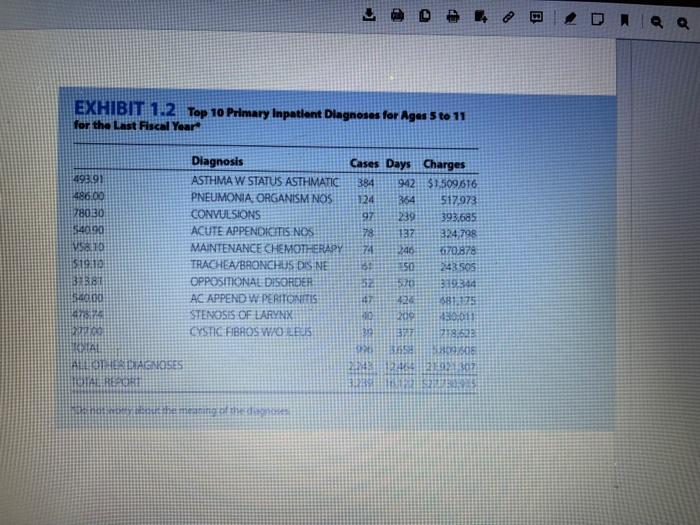
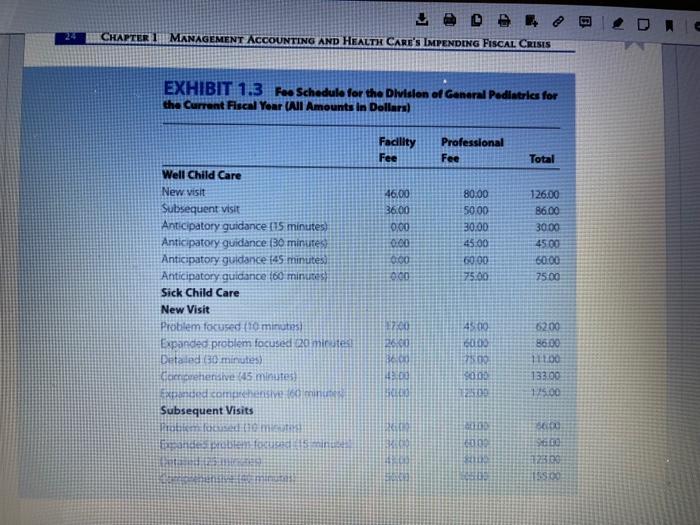
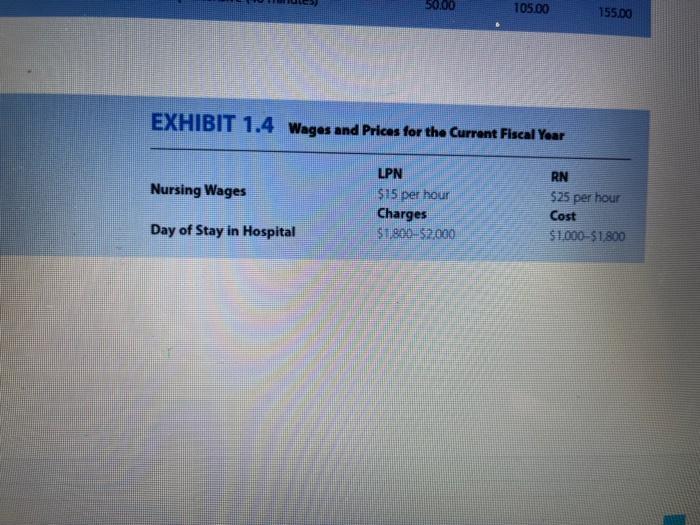
she 4. How should Dr. Lopez translate her budget into a capitation rate that can propose to Continental? What other issues should she consider in her proposal to Continental? 5. What issues should Dr. Lopez consider in working with the PHO, the hospital, and the specialists needed to care for pediatric patients so that she can increase the probability of meeting her budget? PRACTICE CASE CENTRAL VALLEY PRIMARY CARE ASSOCIATES I've got a week to finish this proposal. The information the hospital gave me on Inpatient utilization was incomplete and so detailed that I had to have it sum- marized. Even so, I don't know if I'll be able to use it. How am I supposed to work with information like this to come up with a reasonable capitation rate for Continental? B The speaker was Maria Lopez, MD, board member of Central Valley Primary Care Associates (CVPCA) and chair of its subcommittee on finance, compensation, and risk CVPCA was an independent practice association comprising 130 primary care pediatri- cians who worked in thirty-nine small group practices, located at fifty-seven sites. It worked closely with the Valley Children's Medical Center (VCMC) physician-hospital orga- nization (PHO) Background VCMC was a reaching and research institution (with over 200 beds) that was considered to be one of the leading children's hospitais in the country Ho er, although it had a O Home Search ins A M 2 CHAPTER 1 MANAGEMENT ACCOUNTING AND HEALTH CARE'S IMPENDING FISCAL CRISIS national reputation and was the only children's hospital in the three-state area surround- ing the Central Valley region, it was not the only institution providing pediatric services. Several general hospitals were located nearby, each of which had a small (ten-to thirty- bed) pediatrics department. Moreover, whereas VCMC had both a residency program and an active research agenda, none of the other hospitals was engaged in either teaching or research. Patients in these other hospitals' had relatively uncomplicated diagnoses, requiring fairly standard treatment or procedures. Patients with complicated diagnoses or severe conditions generally were taken directly to VCMC or transported there shortly after admission to one of the other hospitals. Central Valley Primary Care Associates CVPCA had been formed several years ago. Its mission was to develop a comprehensive, integrated primary health care delivery system to ensure quality and cost-effective care. Together with VCMC, it aimed to meet the total health care needs of children and ado- lescents in the tristate area Dr. Lopez's subcommittee was one of six. Its charge was to "develop minimally acceptable capitation fees and fee for service compensation pack- ages that directly correspond to the contractually covered services, and to outline accept- able risk components that may be included in the physician compensation program, such as withholds, risk pool sharing, and maximum stop-loss coverage" develop minimally acceptable capitation fees and fee-for-service compensation pack- ages that directly correspond to the contractually covered services, and to outline accept- able risk components that may be included in the physician compensation program, such as withholds, risk pool sharing, and maximum stop-loss coverage. Continental Health Care Request for Proposals CVPCA originally had planned to contract with the PHO to provide community physicians for primary care. Recently, however, it had received a request for proposals from Conti- nental Health Care, a large managed care plan, indicating that Continental intended to do business with primary care providers on a capitation basis rather than using the tra- ditional fee-for-service approach. All primary care groups in the region had been asked to submit bids specifying the per member, per month amount they would charge Con- tinental for a full-risk contract that is, a contract that included the cost of all primary care, specialty care, and inpatient hospitalization care. Follow-up home health care and specialized services, such as occupational therapy, were excluded. The full range of inpa- tient services was to be included, however, including such traditionally expensive proce- dures as bone marrow transplants Continental had made it clear that it would not be awarding contracts to all groups in the area. Instead, it had said that it would focus its business on the groups that offered the best PMPM rates Inasmuch as Continental currently had contracts that covered some 40 percent of the employees and their families in the region and was growing rapidly, failure to secure a contract would have serious financial implications for la physician group Analysis In an effort to develop a budget and, ultimately, a PMPM rate, Dr. Lopez had asked her staff assistant, Tim Matthews, to gather all the relevant data that she would need to prepare a bid. She had decided to focus her efforts on a small subset of the total analysis. work out the methodology, and then instruct Mr. Matthews to use that methodology for the rest of the analysis. She commented on the rationale for her approach: I have to keep the job manageable. Any time I spend on this is time away from seeing patients. Also, I'm not an accountant, and have no desire to be one. However, Tim doesn't have the clinical knowledge he needs to figure out a methodology. So I decided to focus on children in the five- to eleven year age group and to analyze the cost of their care for the three most frequent outpa- tient diagnoses and the three most frequent inpatient diagnoses. I figure that if I can develop a methodology for this set of children and activities, it'll be a relatively simple matter for Tim to extend the analysis to the whole practice. Because physicians in the group frequently used VCMC's facilities and specialists for outpatient care. Dr. Lopez and Mr. Matthews had assumed that the hospital would be able to supply them with both outpatient and inpatient information. Indeed, Matt Barbert the manager of marketing services for the hospital, had been extremely cooperative He had supplied them with information on outpatient and inpatient diagnoses by age group. a fee schedule for the division of general pediatrics and nursing wages and hospital charges and costs (contained in exhibits 1.1 through 14). He also gave them a list of the aboratory tests radiology procedures, and pharmacy prescriptions that were associated with each inpatient diagnosis mitral fint the en DR relatively simple matter for Tim to extend the analysis to the whole practice. Because physicians in the group frequently used VCMC's facilities and specialists for outpatient care, Dr. Lopez and Mr. Matthews had assumed that the hospital would be able to supply thern with both outpatient and inpatient information. Indeed, Matt Barberi, the manager of marketing services for the hospital, had been extremely cooperative. He had supplied them with information on outpatient and inpatient diagnoses by age group; a fee schedule for the division of general pediatrics; and nursing wages and hospital charges and costs (contained in exhibits 1.1 through 1.4). He also gave them a list of the laboratory tests, radiology procedures, and pharmacy prescriptions that were associated with each inpatient diagnosis. There were two complications with the data Mr. Barberi had submitted. First, the list of tests, procedures, and prescriptions totaled ten to fifteen pages per diagnosis Dr. Lopez realized that working with such a long list for more than a few diagnoses would be extremely cumbersome Under her guidance, Mr Matthews had summarized the informa- tion according to the categories shown in exhibit 15. The second complication was that Mr. Barberi had sent a letter along with the data that had not been especially encouraging. It read, in part As you notice, there are some limitations to the data we have readily available. For example, on the outpatient side, we currently cannot be diagnosis codes with resource utilization. Also, we cannot the diagnosis with the kind and number of specialist referrals or consults. It was this letter that prompted Dr. Lopez's comment at the beginning of the case, and that led her to conclude that whatever analein she died would be based on a wide variety of assumptions. Nevertheless, the sian to densitive ater than to push head EXHIBIT 1.1 Top 3 Outpatient Diagnoses for Ages 5 to 11 for the First 6 Months of the Current Fiscal Year Diagnosis ROUTINE CHILD HEALTH EXAM CHR OTITIS MEDIA NOS/NEC ABN CLINICAL FINDING NEC TOTAL Cases 1.435 1.160 1.104 3,699 "Do not worry about the meaning of the diagnoses 42 180% 1450 38% Percentage of Total Home ASSIGNMENT 23 Search DA E EXHIBIT 1.2 Top 10 Primary Inpatient Diagnoses for Ages 5 to 11 for the Last Fiscal Year 493.91 486.00 78030 $40.90 58.10 $19:10 31381 $40.00 47574 120100 IRONIAL ALL OTHER DIAGNOSES TAL REPORT HOME PNEUMONIA ORGANISM NOS CONVULSIONS Diagnosis Cases Days Charges ASTHMA W STATUS ASTHMATIC 384 942 $1,509,616 124 364 517.973 97 239 393.685 78 137 324,798 74 246 670.878 151 350 243 505 520 ACUTE APPENDICITIS NOS MAINTENANCE CHEMOTHERAPY TRACHEA/BRONCHUS DIS NE C OPPOSITIONAL DISORDER AC APPEND W PERITONITIS STENOSIS OF LARYNX CYSTIC FIBROS WOLBUS meaning of the diagnoses 48 424 1209 13517 315344 $81.375 430,011 1778:628 33095016 320 1358 212548 1464 21921 307 31289 DAQ Q 24 LODE CHAPTER 1 MANAGEMENT ACCOUNTING AND HEALTH CARE'S IMPENDING FISCAL CRISIS EXHIBIT 1.3 Fee Schedule for the Division of General Pediatrics for the Current Fiscal Year (All Amounts in Dollars) Well Child Care New visit Subsequent visit Anticipatory guidance (15 minutes) Anticipatory guidance (30 minutes) Anticipatory guidance (45 minutes) Anticipatory guidance (60 minutes) Sick Child Care New Visit Problem focused (10 minutes) Expanded problem focused 20 minutes! Detailed (30 minutes) Comprehensive (45 minutes) Expanded com hensive (60 minutes Subsequent Visits Expande BOMBER oblem focused (15 minutes MEAN BER Facility Fee 46.00 36.00 0:00 0:00 0:00 0:00 2013 12600 Seco 14303 BELENS Professional Fee 80.00 50.00 30.00 45.00 60.00 75.00 45.00 15000 17500 15000 125.330 FRIEN 6000 BRITIS Total 126.00 86.00 30.00 45.00 60:00 75.00 62.00 86.00 111.00 133.00 1/5.00 5600 S600 125.00 155.00 Nursing Wages 50.00 EXHIBIT 1.4 Wages and Prices for the Current Fiscal Year Day of Stay in Hospital 105.00 LPN $15 per hour Charges $1,800-$2,000 155.00 RN $25 per hour Cost $1,000-$1,800
Step by Step Solution
There are 3 Steps involved in it
Step: 1
Question 4 To translate her budget into a capitation rate that she can propose to Continental Dr Lopez should consider the following steps 1 Identify the total costs incurred by CVPCA for providing he...
Get Instant Access to Expert-Tailored Solutions
See step-by-step solutions with expert insights and AI powered tools for academic success
Step: 2

Step: 3
Ace Your Homework with AI
Get the answers you need in no time with our AI-driven, step-by-step assistance
Get Started
Operations and Supply Chain Management The Core
Authors: Robert Jacobs, Richard Chase, Jaydeep Balakrishnan, Brent Snider
2nd Canadian edition
1259066606, 978-1259066603