All the required info is given below
 All the relevant information is given below
All the relevant information is given below
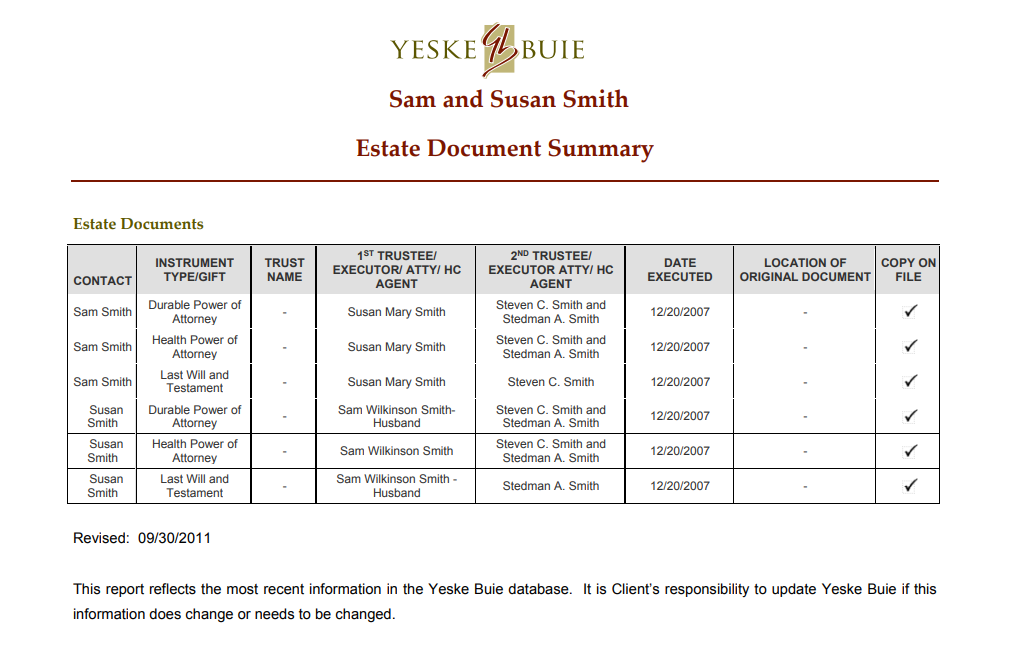
Husband - Health Care Power of Attorney
Husband - Last Will and Testament
Husband -Power of Attorney
Heading 1: The Main Title
Heading 1: The Main Title
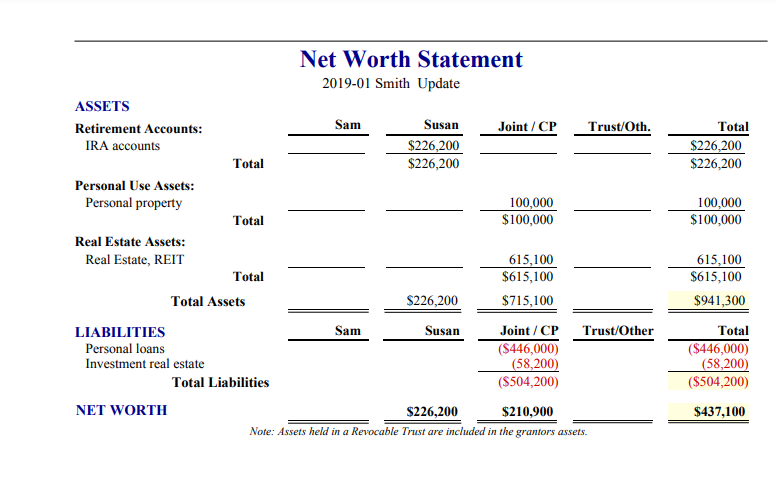
Smiths Net worth Statement
Wife - Health Care Power of Attorney
Wife - Last Will and Testament
Wife - Power of Attorney
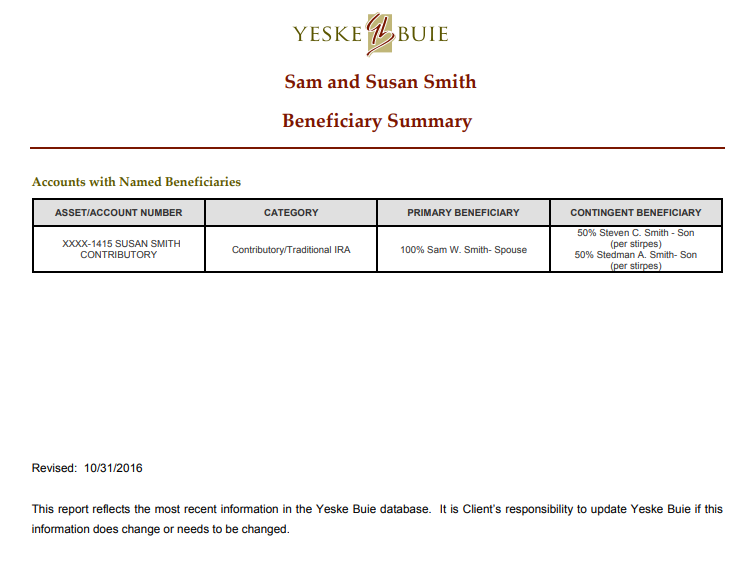
Diagram an estate distribution at the first death and the second death Below is a real fact pattern for real people (names changed, obviously). Please diagram (a hand drawn picture, scanned, is fine; this also works well in excel) how this estate would be distributed at the first death (assume the husband dies first, the men always seem to get picked on in this way) and then at the second death. Assume your purpose is to put together a diagram to use to help these Clients understand their estate distribution scenario. [We do this in real life at Yeske Buie, and you would be AMAZED how often Clients look at the completed diagram and say something like, "What? That isn't what I want to have happen."] Be sure to indicate HOW the assets will pass (e.g. probate, beneficiary, intestate rules, etc.) HEALTH CARE POWER OF ATTORNEY 1. Designation of health care agent. I, Sam Wilkinson Smith, being of sound mind, hereby appoint Name: Susan Mary Smith Home Address: Somewhere, NC Cell Telephone Number: 123-456-7890 as my health care attorney-in-fact (herein referred to as my "health care agent") to act for me and in my name in any way I could act in person) to make health care decisions for me as authorized in this document. If the person named as my health care agent is not reasonably available or is unable or unwilling to act as my agent, then I appoint the following person(s) (each to act alone and successively, in the order named), to serve in that capacity: Name: Steven C. Smith Home Address: Somewhere else, NC Home Telephone Number: 234-567-8901 Name: Stedman A. Smith Home Address: Elsewhere, NC Home Telephone Number: 345-678-9012 Each successor health care agent designated shall be vested with the same power and duties as if originally named as my health care agent. 2. Effectiveness of appointment. Notice: This health care power of attorney may be revoked by you at any time in any manner by which you are able to communicate your intent to revoke to your health care agent and your attending physician Absent revocation, the authority granted in this document shall become effective when and if the physician or physicians designated below determine that I lack sufficient understanding or capacity to make or communicate decisions relating to my health care and will continue in effect during my incapacity, until my death, except if I authorize my health care agent to exercise my rights with respect to anatomical gifts, autopsy, or disposition of my remains, this authority will continue after my death to the extent necessary to exercise the authority granted in this document for these purposes. This determination shall be made by the following physician or physicians for decisions related to mental health treatment, this determination shall be made by the following physician or eligible psychologist. You may include here a designation of your choice, including your attending physician or eligible psychologist, or any other physician or eligible psychologist. You may also name two or more physicians or eligible psychologists, if desired, both of whom must make this determination before the authority granted to the health care agent becomes effective. ANY ATTENDING PHYSICIAN 3. General statement of authority granted. Except as indicated in section 4 below, I hereby grant to my health care agent named above full power and authority to make health care decisions, including mental health treatment decisions, on my behalf, including, but not limited to, the following: A. To request, review, and receive any information, verbal or written, regarding my physical or mental health, including, but not limited to, medical and hospital records, and to consent to the disclosure of this information. B. To employ or discharge my health care providers. C. To consent to and authorize my admission to and discharge from a hospital, nursing or convalescent home, or other institution. D. To consent to and authorize my admission to and retention in a facility for the care or treatment of mental illness. E. To consent to and authorize the administration of medications for mental health treatment and electroconvulsive treatment (ECT) commonly referred to as "shock treatment". F. To give consent for, to withdraw consent for, or to withhold consent for, X ray, anesthesia, medication, surgery, and all other diagnostic and treatment procedures ordered by or under the authorization of a licensed physician, dentist, or podiatrist. This authorization specifically includes the power to consent to measures for relief of pain. G. To authorize the withholding or withdrawal of life-sustaining procedures when and if my physician determines that I am terminally ill, permanently in a coma, suffer severe dementia, or am in a persistent vegetative state. Life-sustaining procedures are those forms of medical care that only serve to artificially prolong the dying process and may include mechanical ventilation, dialysis, antibiotics, artificial nutrition and hydration, and other forms of medical treatment which sustain, restore or supplant vital bodily functions. Life-sustaining procedures do not include care necessary to provide comfort or alleviate pain. I DESIRE THAT MY LIFE NOT BE PROLONGED BY LIFE-SUSTAINING PROCEDURES IF I AM TERMINALLY ILL, PERMANENTLY IN A COMA, SUFFER SEVERE DEMENTIA, OR AM IN A PERSISTENT VEGETATIVE STATE. H. To exercise any right I may have to make a disposition of any part or all of my body for medical purposes; to authorize an autopsy; to make an anatomical gift of my organs or body, or part thereof, and to direct the disposition of my remains. I. To take any lawful actions that may be necessary to carry out these decisions, including the granting of releases of liability to medical providers. 4. Special provisions and limitations. Notice: The above grant of power is intended to be as broad as possible so that your health care agent will have authority to make any decisions you could make to obtain or terminate any type of health care. If you wish to limit the scope of your health care agent's powers, you may do so in this section) A. In exercising the authority to make health care decisions on my behalf, the authority of my health care agent is subject to the following special provisions and limitations (Here you may include any specific limitations you deem appropriate such as: your own definition of when life- sustaining treatment should be withheld or discontinued, or instructions to refuse any specific types of treatment that are inconsistent with your religious beliefs, or unacceptable to you for any other reason.): B. In exercising the authority to make mental health decisions on my behalf, the authority of my health care agent is subject to the following special provisions and limitations. (Here you may include any specific limitations you deem appropriate such as: limiting the grant of authority to make only mental health treatment decisions, your own instructions regarding the administration or withholding of psychotropic medications and electroconvulsive treatment (ECT), instructions regarding your admission to and retention in a health care facility for mental health treatment, or instructions to refuse any specific types of treatment that are unacceptable to you): a C. (Notice: This health care power of attorney may incorporate or be combined with an advance instruction for mental health treatment, executed in accordance with Part 2 of Article 3 of Chapter 122C of the General Statutes, which you may use to state your instructions regarding mental health treatment in the event you lack sufficient understanding or capacity to make or communicate mental health decisions. Because your health care agent's decisions about decisions must be consistent with any statements you have expressed in an advance instruction, you should indicate here whether you have executed an advance instruction for mental health treatment.): D. In exercising the authority to make decisions regarding autopsy, anatomical gifts and disposition of remains on my behalf, the authority of my health care agent is subject to the following special provisions and limitations. (Here you may include any specific limitations you deem appropriate such as: limiting the grant of authority and the scope of authority, instructions regarding gifts of the body or body part, or instructions regarding burial or cremation): 5. Guardianship provision. If it becomes necessary for a court to appoint a guardian of my person, I nominate my health care agent acting under this document to be the guardian of my person, to serve without bond or security. The guardian shall act consistently with G.S. 35A-1201(a)(S). 6. Reliance of third parties on health care agent. A. No person who relies in good faith upon the authority of or any representations by my health care agent shall be liable to me, my estate, my heirs, successors, assigns, or personal representatives, for actions or omissions by my health care agent. B. The powers conferred on my health care agent by this document may be exercised by my health care agent alone, and my health care agent's signature or act under the authority granted in this document may be accepted by persons as fully authorized by me and with the same force and effect as if I were personally present, competent, and acting on my own behalf. All acts performed in good faith by my health care agent pursuant to this power of attorney are done with my consent and shall have the same validity and effect as if I were present and exercised the powers myself, and shall inure to the benefit of and bind me, my estate, my heirs, successors, assigns, and personal representatives. The authority of my health care agent pursuant to this power of attorney shall be superior to and binding upon my family, relatives, friends, and others. 7. Miscellaneous provisions. A. I revoke any prior health care power ofattorney. B. My health care agent shall be entitled to sign, execute, deliver, and acknowledge any contract or other document that may be necessary, desirable, convenient, or proper in order to exercise and carry out any of the powers described in this document and to incur reasonable costs on my behalf incident to the exercise of these powers; provided, however, that except as shall be necessary in order to exercise the powers described in this document relating to my health care, my health care agent shall not have any authority over my property or financial affairs. C. My health care agent and my health care agent's estate, heirs, successors, and assigns are hereby released and forever discharged by me, my estate, my heirs, successors, and assigns and personal representatives from all liability and from all claims or demands of all kinds arising out of the acts or omissions of my health care agent pursuant to this document, except for willful misconduct or gross negligence. D. No act or omission of my health care agent, or of any other person, institution, or facility acting in good faith in reliance on the authority of my health care agent pursuant to this health care power of attorney shall be considered suicide, nor the cause of my death for any civil or criminal purposes, nor shall it be considered unprofessional conduct or as lack of professional competence. Any person, institution, or facility against whom criminal or civil liability is asserted because of conduct authorized by this health care power of attorney may interpose this document as a defense. 8. Signature of principal. By signing here, I indicate that I am mentally alert and competent, fully informed as to the contents s f this document, and understand the full import of this grant of powers to my health care agent. DATE December 20, 2007 9. Signatures of Witnesses. I hereby state that the Principal, Sam Wilkinson Smith, being of sound mind, signed the foregoing health care power of attorney in my presence, and that I am not related to the principal by blood or marriage, and I would not be entitled to any portion of the estate of the principal under any existing will or codicil of the principal or as an heir under the Intestate Succession Act, if the principal died on this date without a will. I also state that I am not the principal's attending physician, nor an employee of the principal's attending physician, nor an employee of the health facility in which the principal is a patient, nor an employee of a nursing home or any group care home where the principal resides. I further state that I do not have any claim against the principal Date:December 20, 2007 Date:December, 20, 2007 Page 5 of 5 STATE OF NORTH CAROLINA COUNTY CERTIFICATE 1. Jane Notary, a Notary Public for Greenville County, North Carolina, hereby certify that Sam Wilkinson Smith appeared before me and swore to me and to the witnesses in my presence that this instrument is a health care power of attorney, and that he/she willingly and voluntarily made and executed it as his/her free act and deed for the purposes expressed in it. I further certify that Mr. Witness and Mrs. Witness, witnesses, appeared before me and swore that they witnessed Sam Wilkinson Smith sign the attached health care power of attorney, believing him/her to be of sound mind; and also swore that at the time they witnessed the signing (i) they were not related within the third degree to him/her or his/her spouse, and (ii) they did not know nor have a reasonable expectation that they would be entitled to any portion of his/her estate upon his/her death under any will or codicil thereto then existing or under the Intestate Succession Act as it provided at that time, and (iii) they were not a physician attending him/her, nor an employee of an attending physician, nor an employee of a health facility in which he/she was a patient, nor an employee of a nursing home or any group-care home in which he/she resided, and (iv) they did not have a claim against him/her. I further certify that I am satisfied as to the genuineness and due execution of the instrument. This the 20th day of December, 2007. Jane Notary Notary Public My Commission Expires: September 6, 2008 LAST WILL AND TESTAMENT of SAM WILKINSON SMITH STATE OF NORTH CAROLINA 1, Sam Wilkinson Smith, being a resident of Greenville County, North Carolina, hereby revoking all former wills made by me declare this to be my Last Will and Testament in the manner and form as follows: ARTICLE I I direct my Executor hereafter named to pay all of my just debts, my funeral expenses and the cost of administration of my estate and to erect at my grave such marker as he or she may deem proper. I further provide that my Executor pay from the general funds of my estate all estate, inheritance and succession taxes, and that my Executor shall not require any transferee, beneficiary, or devisee under this my Last Will and Testament to reimburse my estate for said taxes so paid, nor shall he or she deduct same from the share of any beneficiaries hereunder. ARTICLE II I give, devise and bequeath all of my property of every nature whatsoever and wherever situated to my wife, Susan Mary Smith. ARTICLE III If my said wife shall predecease me, or in the event that my said wife and I shall perish through some common accident or catastrophe, then in either of said events, I give, devise and bequeath all of my property of every nature whatsoever and wherever situated in equal shares to my two children, viz: Stedman A. Smith and Steven C. Smith. ARTICLE TV I appoint my wife, Susan Mary Smith, to be the Executrix of this my Last Will and Testament; and I vest my said Executrix with full power and authority to sell, transfer and convey any property, real or personal, which I may own at the time of my death at such time and price and upon such terms and conditions, including credit, as she may determine and to do every other act and thing necessary or appropriate for the complete administration of my estate. Without in any way limiting the generality of the foregoing provision, I hereby grant my Executrix all of the powers set forth in North Carolina General Statutes, Section 32-27, subject to the powers set forth in North Carolina General Statutes, Section 32-26 and these powers are incorporated by reference. If my said wife shall predecease me or for any reason shall fail to qualify as Executrix hereunder, or having qualified, shall die or resign, then in such event, Steven C. Smith, shall act as Executor of my estate and in such capacity shall possess and exercise all powers and authority herein conferred on my said wife and as Executrix. 1. Sam Wilkinson Smith, the Testator, sign my name to this instrument this 20 day of December, 2007, and being first duly sworn, declare to the undersigned authority that I sign and execute this instrument as my last will and that I sign it willingly, that I execute it as my free and voluntary act for the purposes therein expressed, and that I am eighteen years of age or older, of sound mind, and under no constraint or undue influ We, the undersigned witnesses, sign our names to this instrument, being first duly sworn, and do hereby declare to the undersigned authority that the Testator signs and executes this instrument as his last will and that he signs it willingly, and that each of us, in the presence and hearing of the Testator, hereby signs this will as witness to the Testator's signing, and that to the best of our knowledge the Testator is eighteen years of age or older, of sound mind, and under no constraint or undue influence. Witness Witness STATE OF NORTH CAROLINA Subscribed, sworn to and acknowledged before me by Sam Wilkinson Smith, Testator, and subscribed and swom to before me by Mr. Witness and Mrs. Witness, witnesses, this 20th day of December, 2007. Jane Notary, Notary Public My Commission expires: September 6, 2008 Prepared by and Return to: The Law Office of Jones & Shapiro, PA 123 North Main Street Greenville, NC 28115 STATE OF NORTH CAROLINA COUNTY OF GREENVILLE POWER OF ATTORNEY 1, Sam Wilkinson Smith, of Greenville County, North Carolina, revoking all Powers-of Attorney previously executed by me, hereby appoint Susan Mary Smith, as my attorney-in-fact (herein "my attorney") to act in my name, place and stead in any way which I could act if I were personally present with respect to the following matters: (!) To buy, lease, exchange or otherwise acquire and to contract for the purchase, lease, exchange and acquisition of, and to accept, receive and possess any interest in real property, wherever located, on such terms and conditions as my attorney shall deem proper, to gift, sell, exchange, lease, subdivide, partition, mortgage, subject to liens, subject to deeds of trust or otherwise encumber any interest in real property now owned by me or hereafter acquired, on such terms and conditions as my attorney shall deem proper; to repair, rebuild, improve, insure, maintain and otherwise manage any interest in real property now owned or hereafter acquired by me on such terms and conditions as my attorney shall deem proper. (2) To accept, receive, possess, purchase, exchange, lease or otherwise acquire and to contract for the purchase, exchange, lease or acquisition of personal property, tangible or intangible on such terms and conditions as my attorney shall deem proper; to maintain, repair, insure, lease, sell, hypothecate, subject to liens, mortgage, encumber, store, and otherwise manage any personal property, wherever located, tangible or intangible, that I now own or hereafter acquire on such terms and conditions as my attorney deems proper. (3) To make, receive, sign, endorse, execute, acknowledge, deliver and possess checks, drafts, bills of exchange, letters of credit, notes, stock certificates, other negotiable instruments of any character, withdrawal receipts and deposit instruments relating to accounts or deposits in or certificates of deposit of banks, savings and loan or other institutions or associations on my behalf whether such accounts, deposits or certificates are in my own name or held jointly with another. (4) To enter into any safe deposit box to which Ihave access. (5) To receive, hold and possess all legacies, bequests and devises as are now owned by, due, owing, payable or belonging to me. (6) To exercise or perform any act, power, duty, right or obligation whatsoever in regard to any contract of life, accident, health, disability or liability insurance or any combination of such insurance procured by me or on my behalf. (7) To conduct, or transact any business in which I am engaged. (8) To borrow money in my name in such amount as may be necessary, in my said attorney's sole discretion, to preserve and protect my estate, or any business in which I am engaged and to finance the purchase of U.S. government bonds which are eligible for use to pay federal estate tax; to execute and deliver deeds of trust on real property owned by me and to pledge other assets owned by me to secure the repayment of amounts borrowed; to compromise or refinance any note, mortgage or other indebtedness now or hereafter due by me. (9) To request, ask, demand, sue for, recover, collect and to have, use and take all lawful means and equitable and legal remedies, procedures and writs in my name for the collection and recovery of any property, interest in property and any rights of mine, including all sums of money, debts, dues, accounts, insurance proceeds, legacies, devises, bequests, interest, dividends, annuities and any other interests as are owned by or due, owing, payable or belonging to me (whether such sums are due me from the government of the United States or any subdivision thereof); to adjust, sell, compromise, arbitrate or otherwise agree for me representing the same; to make, execute and deliver for me all endorsements, acquittances, releases, receipts or other sufficient discharges for the same; and to make oaths, acknowledgments and verifications in my name. (10) To pay, adjust and settle any legitimate and just claims or debts which may be due and owing by me at any time; and to credit payment of or cancel any note, mortgage, deed of trust, or other obligation to me upon proper payment being made, whether in full or by way of compromise or settlement, on evidence thereof satisfactory to my attorney being furnished. (11) To prepare, execute and file all social security, unemployment insurance and information returns required by the laws of the United States, or of any state or subdivision thereof, or of any foreign government. (12) To prepare, execute, verify and file in my name and on my behalf any and all types of tax returns, amended returns, declaration of estimated tax, report, protest, application for correction of assessed valuation of real or other property, appeal, brief, claim for refund, or petition, including petition to the Tax Court of the United States, in connection with any tax imposed or proposed to be imposed by any government, or claimed, levied or assessed by any government, and to pay any such tax and to obtain any extension of time for any of the foregoing; to execute waivers or consents agreeing to a later determination and assessment of taxes than is provided by any statute of limitations; to execute waivers of restriction on the assessment and collection of deficiency in any tax; to execute closing agreements and all other documents, instruments and papers relating to any tax liability of any sort; to institute and carry on through counsel any proceeding in connection with determining or contesting any such tax or to recover any tax paid or to resist any claim for additional tax on any proposed assessment or levy thereof; and to enter into any agreements or stipulations for compromise or other adjustments or dispositions of any tax. (13) To invest and reinvest without restriction any of my money or other property of whatever kind coming into its possession or known to belong to me, whether income or principal, in such manner as it may deem fit and proper and to execute any instruments necessary to accomplish these purposes. I hereby authorize it to retain any property owned by me without regard to any requirement of diversification otherwise imposed by law or government regulation and without liability for any loss or decrease in the value of any such property while retained by it and to exercise by proxy or otherwise any voting rights I may have in shares of stock. (14) To employ agents such as legal counsel, accountants or other professional representation as may be appropriate and to grant such agents powers of attorney or their appropriate authorization as may be required in connection with such representation or by the Internal Revenue Service or other governmental authority; to employ investment counsel, brokers, and appraisers as my attorney deems advisable. (15) To engage in health care arrangements and decisions which affect me and are for my benefit including dealing with doctors, nurses, hospitals and others engaged in the health care industry. (16) To make gifts for me or on my behalf including gifts to my named attorney-in-fact which may be for the purpose of estate or tax planning. (17) Generally, to act for me in all matters affecting my business or property, with the same force and effect and to all intents and purposes as though I were personally present and acting for myself. In addition to the foregoing powers I specifically grant my attorney all the powers set forth in Section 32-27 of the North Carolina General Statutes which are hereby incorporated by reference. In addition, I appoint Stedman A. Smith and Steven C. Smith to serve as alternate attorneys-in-fact but without authority to exercise any of the powers set forth above except that if Susan Mary Smith shall be unable or unwilling to serve or to continue to serve as such Attorney, then my alternate attorney shall be fully authorized to serve hereunder, and shall have all of the powers granted originally to my Attorneys, and the term "Attorney" shall thereupon refer to my alternate attorney named herein. My alternate attorney may execute and deliver an affidavit that my Attorney is unwilling or unable to serve or to continue to serve, and such affidavit shall be conclusive evidence insofar as third parties are concerned of the facts set forth therein, and, in such event, any person acting in reliance upon such affidavit shall incur no liability to my estate because of such reliance. All powers and authority given to my said alternate attorneys-in-fact may be exercised, and all things herein set out to be done by them may be done, by any one of them acting alone and without the consent or joinder of the other. I direct that my attorney shall not be required to post a bond or to file with any Court or any public official any report or accounting relating to the administration of my affairs except to the extent that I have no power to excuse the filing of such reports or accounting. My said attorney shall furnish to me annually, or at more frequent intervals, reports and accounts of all actions taken pursuant to the authority herein granted. This Power of Attorney is executed under the authority of Article 2 of Chapter 32A of the North Carolina General Statutes and shall remain in full force and effect until revoked and canceled as provided therein. I hereby revoke any prior Power of Attorney executed by me. This Power of Attorney shall not be affected by my subsequent incapacity or mental incompetence. It may be registered in the office of the Register of Deeds in any given County, North Carolina. I direct that if at any time following the execution of this Power of Attorney, a court appoints a conservator or guardian of my estate, I request that the court making such appointment consider my nomination of my acting attorney-in-fact to serve as such conservator or guardian of my estate. IN TESTIMONY WHEREOF, I have hereunto set my hand and seal, this 20th day of December, 2007. no Grantor) Sam Wilkinson Smith STATE OF NORTH CAROLINA COUNTY OF GREENVILLE 1, Jane Notary, a Notary Public in and for Greenville County, North Carolina, do hereby certify that Sam Wilkinson Smith personally appeared before me on this date and duly acknowledged the execution of the forening instrument for the purposes therein set forth. my hand and notarial Seal, this 20th day of December, 2007. My Commission Expires: September 6, 2008 YESKELBUIE Sam and Susan Smith Beneficiary Summary Accounts with Named Beneficiaries ASSETIACCOUNT NUMBER CATEGORY PRIMARY BENEFICIARY CONTINGENT BENEFICIARY XXXX-1415 SUSAN SMITH CONTRIBUTORY Contributory Traditional IRA 100% Sam W. Smith-Spouse 50% Steven C. Smith - Son (per stirpes) 50% Stedman A. Smith-Son (per stirpes) Revised: 10/31/2016 This report reflects the most recent information in the Yeske Buie database. It is Client's responsibility to update Yeske Buie if this information does change or needs to be changed. YESKELBUIE Sam and Susan Smith Estate Document Summary Estate Documents INSTRUMENT TYPE/GIFT TRUST NAME 1ST TRUSTEE EXECUTORI ATTYI HC AGENT DATE EXECUTED LOCATION OF ORIGINAL DOCUMENT COPY ON FILE CONTACT 2ND TRUSTEE EXECUTOR ATTY/ HC AGENT Steven C. Smith and Stedman A. Smith Steven C. Smith and Stedman A. Smith Sam Smith Susan Mary Smith 12/20/2007 Sam Smith Susan Mary Smith 12/20/2007 Sam Smith Susan Mary Smith Steven C. Smith 12/20/2007 Durable Power of Attorney Health Power of Attorney Last Will and Testament Durable Power of Attorney Health Power of Attorney Last Will and Testament Susan Sam Wilkinson Smith- Husband 12/20/2007 Steven C. Smith and Stedman A. Smith Steven C. Smith and Stedman A. Smith Sam Wilkinson Smith Smith Susan Smith Susan Smith 12/20/2007 Sam Wilkinson Smith Husband Stedman A. Smith 12/20/2007 Revised: 09/30/2011 This report reflects the most recent information in the Yeske Buie database. It is Client's responsibility to update Yeske Buie if this information does change or needs to be changed. YESKELBUIE Sam and Susan Smith Insurance Summary Life Insurance INSURANCE: POLICY NUMBER OR NAME POLICY HOLDER INSURED POLICY TYPE CURRENT DEATH BENEFIT PRIMARY BENEFICIARY SECONDARY BENEFICIARY ANNUAL PREMIUM POLICY ISSUED DATE POLICY ON FILE Sam Smith Sam Smith $250,000 100% Susan Smith: 50% Steven Smith 50% Stedman Smith $5,124 Sam Smith Sam Smith $40.000 100% Susan Smith % $660 Sam's American General Life Insurance Policy Sam's Reliastar Life Insurance Policy Susan's Metropolitan Life Insurance Policy Susan's Kaiser Life Insurance Policy Susan's Prudential Life Insurance Policy Susan Smith Susan Smith $150.000 100% Sam Smith $1,920 Susan Smith Susan Smith $12,500 100% Sam Smith none Susan Smith Susan Smith $10,000 100% Sam Smith $345 Long-Term-Care Insurance POLICY WAITING PERIOD BENEFIT PERIOD MAXIMUM BENEFIT HOME HEALTH CARE BENEFIT INFLATION PROTECTION ANNUAL PREMIUM POLICY ISSUED DATE POLICY ON FILE 90 days 2 years $36,500 $281 6/7/2010 INSURANCE: POLICY INSURED NUMBER OR NAME Sam's John Hancock Long Sam Smith Term Policy Susan's John Hancock Susan Long Term Policy Smith Sam's UNUM Long Term Sam Smith Care Insurance Policy 90 days 5 years $273,750 $1,997 6/7/2010 180 days Unlimited $4,000 per month $ $1,700 3/21/2000 YESKEBUIE Property and Casualty Insurance INSURANCE: POLICY NUMBER OR NAME INSURANCE: RECORD TYPE DEDUCTIBLE LIABILITY ANNUAL PREMIUM POLICY ISSUED DATE POLICY ON FILE USAA Umbrella Policy UMBRELLA 5/19/2001 Total $226,200 $226,200 100,000 $100,000 Net Worth Statement 2019-01 Smith Update ASSETS Retirement Accounts: Sam Susan Joint / CP Trust/Oth. IRA accounts $226,200 Total $226,200 Personal Use Assets: Personal property 100,000 Total $100,000 Real Estate Assets: Real Estate, REIT 615,100 Total $615,100 Total Assets $226,200 $715,100 LIABILITIES Sam Susan Joint / CP Trust/Other Personal loans (5446,000) Investment real estate (58,200) Total Liabilities ($504,200) NET WORTH $226,200 $210,900 Note: Assets held in a Revocable Trust are included in the grantors assets. 615,100 $615,100 $941,300 Total ($446,000) (58,200) ($504,200) $437,100 HEALTH CARE POWER OF ATTORNEY 1. Designation of health care agent. 1, Susan Mary Smith, being of sound mind, hereby appoint: Name: Sam Wilkinson Smith Home Address: Somewhere, NC Telephone Number: 456-789-0123 as my health care attorney-in-fact (herein referred to as my "health care agent") to act for me and in my name in any way I could act in person) to make health care decisions for me as authorized in this document. If the person named as my health care agent is not reasonably available or is unable or unwilling to act as my agent, then I appoint the following person(s) (each to act alone and successively, in the order named), to serve in that capacity: Name: Stedman A. Smith Home Address: Somewhere Else, NC Home Telephone Number: 234-567-8901 Name: Steven C. Smith Home Address: Elsewhere, NC Home Telephone Number: 345-678-9012 Each successor health care agent designated shall be vested with the same power and duties as if originally named as my health care agent. 2. Effectiveness of appointment. Notice: This health care power of attorney may be revoked by you at any time in any manner by which you are able to communicate your intent to revoke to your health care agent and your attending physician Absent revocation, the authority granted in this document shall become effective when and if the physician or physicians designated below determine that I lack sufficient understanding or capacity to make or communicate decisions relating to my health care and will continue in effect during my incapacity, until my death, except if I authorize my health care agent to exercise my rights with respect to anatomical gifts, autopsy, or disposition of my remains, this authority will continue after my death to the extent necessary to exercise the authority granted in this document for these purposes. This determination shall be made by the following physician or physicians For decisions related to mental health treatment, this determination shall be made by the following physician or eligible psychologist. You may include here a designation of your choice, including your attending physician or eligible psychologist, or any other physician or eligible psychologist. You may also name two or more physicians or eligible psychologists, if desired, both of whom must make this determination before the authority granted to the health care agent becomes effective. ANY ATTENDING PHYSICIAN 3. General statement of authority granted. Except as indicated in section 4 below, I hereby grant to my health care agent named above full power and authority to make health care decisions, including mental health treatment decisions, on my behalf, including, but not limited to, the following: A. To request, review, and receive any information, verbal or written, regarding myphysical or mental health, including, but not limited to, medical and hospital records, and to consent to the disclosure of this information. B. To employ or discharge my health care providers. C. To consent to and authorize my admission to and discharge from a hospital, nursing or convalescent home, or other institution. D. To consent to and authorize my admission to and retention in a facility for the care or treatment of mental illness. E. To consent to and authorize the administration of medications for mental health treatment and electroconvulsive treatment (ECT) commonly referred to as "shock treatment". F. To give consent for, to withdraw consent for, or to withhold consent for, X ray, anesthesia, medication, surgery, and all other diagnostic and treatment procedures ordered by or under the authorization of a licensed physician, dentist, or podiatrist. This authorization specifically includes the power to consent to measures for relief of pain. G. To authorize the withholding or withdrawal oflife-sustaining procedures when and if my physician determines that I am terminally ill, permanently in a coma, suffer severe dementia, or am in a persistent vegetative state. Life-sustaining procedures are those forms of medical care that only serve to artificially prolong the dying process and may include mechanical ventilation, dialysis, antibiotics, artificial nutrition and hydration, and other forms of medical treatment which sustain, restore or supplant vital bodily functions. Life-sustaining procedures do not include care necessary to provide comfort or alleviate pain. I DESIRE THAT MY LIFE NOT BE PROLONGED BY LIFE-SUSTAINING PROCEDURES IF I AM TERMINALLY ILL, PERMANENTLY IN A COMA, SUFFER SEVERE DEMENTIA, OR AM IN A PERSISTENT VEGETATIVE STATE. H. To exercise any right I may have to make a disposition of any part or all of my body for medical purposes; to authorize an autopsy; to make an anatomical gift of my organs or body, or part thereof, and to direct the disposition of my remains. 1. To take any lawful actions that may be necessary to carry out these decisions, including the granting of releases of liability to medical providers. 4. Special provisions and limitations. Notice: The above grant of power is intended to be as broad as possible so that your health care agent will have authority to make any decisions you could make to obtain or terminate any type of health care. If you wish to limit the scope of your health care agent's powers, you may do so in this section) A. In exercising the authority to make health care decisions on my behalf, the authority of my health care agent is subject to the following special provisions and limitations (Here you may include any specific limitations you deem appropriate such as: your own definition of when life- sustaining treatment should be withheld or discontinued, or instructions to refuse any specific types of treatment that are inconsistent with your religious beliefs, or unacceptable to you for any other reason.): B. In exercising the authority to make mental health decisions on my behalf, the authority of my health care agent is subject to the following special provisions and limitations. (Here you may include any specific limitations you deem appropriate such as: limiting the grant of authority to make only mental health treatment decisions, your own instructions regarding the administration or withholding of psychotropic medications and electroconvulsive treatment (ECT), instructions regarding your admission to and retention in a health care facility for mental health treatment, or instructions to refuse any specific types of treatment that are unacceptable to you): C. (Notice: This health care power of attorney may incorporate or be combined with an advance instruction for mental health treatment, executed in accordance with Part 2 of Article 3 of Chapter 122C of the General Statutes, which you may use to state your instructions regarding mental health treatment in the event you lack sufficient understanding or capacity to make or communicate mental health treatment decisions. Because your health care agent's decisions about decisions must be consistent with any statements you have expressed in an advance instruction, you should indicate here whether you have executed an advance instruction for mental health treatment.): D. In exercising the authority to make decisions regarding autopsy, anatomical gifts and disposition of remains on my behalf, the authority of my health care agent is subject to the following special provisions and limitations. (Here you may include any specific limitations you deem appropriate such as: limiting the grant of authority and the scope of authority, instructions regarding gifts of the body or body part, or instructions regarding burial or cremation): S. Guardianship provision. If it becomes necessary for a court to appoint a guardian of my person, I nominate my health care agent acting under this document to be the guardian of my person, to serve without bond or security. The guardian shall act consistently with G.S. 35A-1201(a)(5). 6. Reliance of third parties on health care agent. A. No person who relies in good faith upon the authority of or any representations by my health care agent shall be liable to me, my estate, my heirs, successors, assigns, or personal representatives, for actions or omissions by my health care agent. B. The powers conferred on my health care agent by this document may be exercised by my health care agent alone, and my health care agent's signature or act under the authority granted in this document may be accepted by persons as fully authorized by me and with the same force and effect as if I were personally present, competent, and acting on my own behalf. All acts performed in good faith by my health care agent pursuant to this power of attorney are done with my consent and shall have the same validity and effect as ifl were present and exercised the powers myself, and shall inure to the benefit of and bind me, my estate, my heirs, successors, assigns, and personal representatives. The authority of my health care agent pursuant to this power of attorney shall be superior to and binding upon my family, relatives, friends, and others. 7. Miscellaneous provisions. A. I revoke any prior health care power of attorney. B. My health care agent shall be entitled to sign, execute, deliver, and acknowledge any contract or other document that may be necessary, desirable, convenient, or proper in order to exercise and carry out any of the powers described in this document and to incur reasonable costs on my behalf incident to the exercise of these powers; provided, however, that except as shall be necessary in order to exercise the powers described in this document relating to my health care, my health care agent shall not have any authority over my property or financial affairs. C. My health care agent and my health care agent's estate, heirs, successors, and assigns are hereby released and forever discharged by me, my estate, my heirs, successors, and assigns and personal representatives from all liability and from all claims or demands of all kinds arising out of the acts or omissions of my health care agent pursuant to this document, except for willful misconduct or gross negligence. D. No act or omission of my health care agent, or of any other person, institution, or facility acting in good faith in reliance on the authority of my health care agent pursuant to this health care power of attomey shall be considered suicide, nor the cause of my death for any civil or criminal purposes, nor shall it be considered unprofessional conduct or as lack of professional competence. Any person, institution, or facility against whom criminal or civil liability is asserted because of conduct authorized by this health care power of attomey may interpose this document as a defense. 8. Signature of principal. By signing here, I indicate that I am mentally alert and competent, fully informed as to the contents of this document, and understand the full import of this grant of powers to my health care 9. Signatures of Witnesses. I hereby state that the Principal, Susan Mary Smith, being of sound mind, signed the foregoing health care power of attorney in my presence, and that I am not related to the principal by blood or marriage, and I would not be entitled to any portion of the estate of the principal under any existing will or codicil of the principal or as an heir under the Intestate Succession Act, if the principal died on this date without a will. I also state that I am not the principal's attending physician, nor an employee of the principal's attending physician, nor an employee of the health facility in which the principal is a patient, nor an employee of a nursing home or any group care home where the principal resides. I further state that I do not have any claim against the principal. Date: December 20, 2007 Date: December 20, 2007 STATE OF NORTH CAROLINA COUNTY OF Greenville CERTIFICATE I, Jane Notary, a Notary Public for Greenville County, North Carolina, hereby certify that Susan Mary Smith appeared before me and swore to me and to the witnesses in my presence that this instrument is a health care power of attorney, and that he/she willingly and voluntarily made and executed it as his/her free act and deed for the purposes expressed in it. I further certify that Mr. Witness and Mrs. Witness, witnesses, appeared before me and swore that they witnessed Susan Mary Smith sign the attached health care power of attorney, believing him/her to be of sound mind; and also swore that at the time they witnessed the signing (i) they were not related within the third degree to him/her or his/her spouse, and (ii) they did not know nor have a reasonable expectation that they would be entitled to any portion of his/her estate upon his/her death under any will or codicil thereto then existing or under the Intestate Succession Act as it provided at that time, and (iii) they were not a physician attending him/her, nor an employee of an attending physician, nor an employee of a health facility in which he/she was a patient, nor an employee of a nursing home or any group-care home in which he/she resided, and (iv) they did not have a claim against him/her. I further certify that I am satisfied as to the genuineness and due execution of the instrument. This the 20th day of December, 2007. Jane Notary Notary Public My Commission Expires: September 6, 2008 LAST WILL AND TESTAMENT of SUSAN MARY SMITH STATE OF NORTH CAROLINA I. Susan Mary Smith, being a resident of Greenville County, North Carolina, hereby revoking all former wills made by me declare this to be my Last Will and Testament in the manner and form as follows: ARTICLE I I direct my Executor hereafter named to pay all of my just debts, my funeral expenses and the cost of administration of my estate and to erect at my grave such marker as he or she may deem proper. I further provide that my Executor pay from the general funds of my estate all estate, inheritance and succession taxes, and that my Executor shall not require any transferee, beneficiary, or devisee under this my Last Will and Testament to reimburse my estate for said taxes so paid, nor shall he or she deduct same from the share of any beneficiaries hereunder. ARTICLE II I give, devise and bequeath all of my property of every nature whatsoever and wherever situated to my husband, Sam Wilkinson Smith. ARTICLE II If my said husband shall predecease me, or in the event that my said husband and I shall perish through some common accident or catastrophe, then in either of said events, I give, devise and bequeath all of my property of every nature whatsoever and wherever situated in equal shares to my two children, viz: Stedman A. Smith and Steven C. Smith. ARTICLE IV I appoint my husband, Sam Wilkinson Smith, to be the Executor of this my Last Will and Testament; and I vest my said Executor with full power and authority to sell, transfer and convey any property, real or personal, which I may own at the time of my death at such time and price and upon such terms and conditions, including credit, as he may determine and to do every other act and thing necessary or appropriate for the complete administration of my estate. Without in any way limiting the generality of the foregoing provision, I hereby grant my Executor all of the powers set forth in North Carolina General Statutes, Section 32-27, subject to the powers set forth in North Carolina General Statutes, Section 32-26 and these powers are incorporated by reference. If my said husband shall predecease me or for any reason shall fail to qualify as Executor hereunder, or having qualified, shall die or resign, then in such event, Stedman A. Smith, shall act as Executor of my estate and in such capacity shall possess and exercise all powers and authority herein conferred on my said husband and as Executor. i4 I, Susan Mary Smith, the Testatrix, sign my name to this instrument this :20-day of December, 2007, and being first duly sworn, declare to the undersigned authority that I sign and execute this instrument as my last will and that I sign it willingly, that I execute it as my free and voluntary act for the purposes therein expressed, and that I am eighteen years of age or older, of sound mind, and under no constraint or undue influence. We, the undersigned witnesses, sign our names to this instrument, being first duly sworn, and do hereby declare to the undersigned authority that the Testatrix signs and executes this instrument as her last will and that she signs it willingly, and that each of us, in the presence and hearing of the Testatrix, hereby signs this will as witness to the Testatrix's signing, and that to the best of our knowledge the Testatrix is eighteen years of age or older, of sound mind, and under no constraint or undue influence. Witness Witness STATE OF NORTH CAROLINA COUNTY OF GREENVILLE Subscribed, sworn to and acknowledged before me by Susan Mary Smith, Testatrix, and subscribed and swom to before me by Mr. Witness and Mrs. Witness, witnesses, this 20th day of December, 2007. Jane Notary, Notary Public My Commission expires: September 6, 2008 Prepared by and Return to: The Law Office of Jones & Shapiro, PA 123 North Main Street Greenville, NC 28115 STATE OF NORTH CAROLINA COUNTY OF GREENVILLE POWER OF ATTORNEY 1, Susan Mary Smith, of Greenville County, North Carolina, revoking all Powers-of Attorney previously executed by me, hereby appoint Sam Wilkinson Smith, as my attorney-in-fact (herein "my attorney") to act in my name, place and stead in any way which I could act if I were personally present with respect to the following matters: (1) To buy, lease, exchange or otherwise acquire and to contract for the purchase, lease, exchange and acquisition of, and to accept, receive and possess any interest in real property, wherever located, on such terms and conditions as my attorney shall deem proper; to gift, sell, exchange, lease, subdivide, partition, mortgage, subject to liens, subject to deeds of trust or otherwise encumber any interest in real property now owned by me or hereafter acquired, on such terms and conditions as my attorney shall deem proper; to repair, rebuild, improve, insure, maintain and otherwise manage any interest in real property now owned or hereafter acquired by me on such terms and conditions as my attorney shall deem proper. (2) To accept, receive, possess, purchase, exchange, lease or otherwise acquire and to contract for the purchase, exchange, lease or acquisition of personal property, tangible or intangible on such terms and conditions as my attorney shall deem proper; to maintain, repair, insure, lease, sell, hypothecate, subject to liens, mortgage, encumber, store, and otherwise manage any personal property, wherever located, tangible or intangible, that I now own or hereafter acquire on such terms and conditions as my attorney deems proper. (3) To make, receive, sign, endorse, execute, acknowledge, deliver and possess checks, drafts, bills of exchange, letters of credit, notes, stock certificates, other negotiable instruments of any character, withdrawal receipts and deposit instruments relating to accounts or deposits in or certificates of deposit of banks, savings and loan or other institutions or associations on my behalf whether such accounts, deposits or certificates are in my own name or held jointly with another. (4) To enter into any safe deposit box to which I have access. (5) To receive, hold and possess all legacies, bequests and devises as are now owned by, due, owing, payable or belonging to me. (6) To exercise or perform any act, power, duty, right or obligation whatsoever in regard to any contract of life, accident, health, disability or liability insurance or any combination of such insurance procured by me or on my behalf. (7) To conduct, or transact any business in which I am engaged. (8) To borrow money in my name in such amount as may be necessary, in my said attorney's sole discretion, to preserve and protect my estate, or any business in which I am engaged and to finance the purchase of U.S. government bonds which are eligible for use to pay federal estate tax; to execute and deliver deeds of trust on real property owned by me and to pledge other assets owned by me to secure the repayment of amounts borrowed; to compromise or refinance any note, mortgage or other indebtedness now or hereafter due by me. (9) To request, ask, demand, sue for, recover, collect and to have, use and take all lawful means and equitable and legal remedies, procedures and writs in my name for the collection and recovery of any property, interest in property and any rights of mine, including all sums of money, debts, dues, accounts, insurance proceeds, legacies, devises, bequests, interest, dividends, annuities and any other interests as are owned by or due, owing, payable or belonging to me (whether such sums are due me from the government of the United States or any subdivision thereof); to adjust, sell, compromise, arbitrate or otherwise agree for me representing the same; to make, execute and deliver for me all endorsements, acquittances, releases, receipts or other sufficient discharges for the same; and to make oaths, acknowledgments and verifications in my name. (10) To pay, adjust and settle any legitimate and just claims or debts which may be due and owing by me at any time; and to credit payment of or cancel any note, mortgage, deed of trust, or other obligation to me upon proper payment being made, whether in full or by way of compromise or settlement, on evidence thereof satisfactory to my attorney being furnished. (11) To prepare, execute and file all social security, unemployment insurance and information returns required by the laws of the United States, or of any state or subdivision thereof, or of any foreign government. (12) To prepare, execute, verify and file in my name and on my behalf any and all types of tax returns, amended returns, declaration of estimated tax, report, protest, application for correction of assessed valuation of real or other property, appeal, brief, claim for refund, or petition, including petition to the Tax Court of the United States, in connection with any tax imposed or proposed to be imposed by any government, or claimed, levied or assessed by any government, and to pay any such tax and to obtain any extension of time for any of the foregoing; to execute waivers or consents agreeing to a later determination and assessment of taxes than is provided by any statute of limitations; to execute waivers of restriction on the assessment and collection of deficiency in any tax; to execute closing agreements and all other documents, instruments and papers relating to any tax liability of any sort; to institute and carry on through counsel any proceeding in connection with determining or contesting any such tax or to recover any tax paid or to resist any claim for additional tax on any proposed assessment or levy thereof; and to enter into any agreements or stipulations for compromise or other adjustments or dispositions of any tax. (13) To invest and reinvest without restriction any of my money or other property of whatever kind coming into its possession or known to belong to me, whether income or principal, in such manner as it may deem fit and proper and to execute any instruments necessary to accomplish these purposes. I hereby authorize it to retain any property owned by me without regard to any requirement of diversification otherwise imposed by law or government regulation and without liability for any loss or decrease in the value of any such property while retained by it and to exercise by proxy or otherwise any voting rights I may have in shares of stock. (14) To employ agents such as legal counsel, accountants or other professional representation as may be appropriate and to grant such agents powers of attorney or their appropriate authorization as may be required in connection with such representation or by the Internal Revenue Service or other governmental authority; to employ investment counsel, brokers, and appraisers as my attorney deems advisable. (15) To engage in health care arrangements and decisions which affect me and are for my benefit including dealing with doctors, nurses, hospitals and others engaged in the health care industry. (16) To make gifts for me or on my behalf including gifts to my named attorney-in-fact which may be for the purpose of estate or tax planning. (17) Generally, to act for me in all matters affecting my business or property, with the same force and effect and to all intents and purposes as though I were personally present and acting for myself. In addition to the foregoing powers I specifically grant my attorney all the powers set forth in Section 32-27 of the North Carolina General Statutes which are hereby incorporated by reference. In addition, I appoint Stedman A. Smith and Steven C. Smith to serve as alternate attorneys-in-fact but without authority to exercise any of the powers set forth above except that if Sam Wilkinson Smith shall be unable or unwilling to serve or to continue to serve as such Attorney, then my alternate attorney shall be fully authorized to serve hereunder, and shall have all of the powers granted originally to my Attorneys, and the term "Attorney" shall thereupon refer to my alterate attorney named herein. My alternate attorney may execute and deliver an affidavit that my Attorney is unwilling or unable to serve or to continue to serve and such affidavit shall be conclusive evidence insofar as third parties are concerned of the facts set forth therein, and, in such event, any person acting in reliance upon such affidavit shall incur no liability to my estate because of such reliance. All powers and authority given to my said alternate attorneys-in-fact may be exercised, and all things herein set out to be done by them may be done, by any one of them acting alone and without the consent or joinder of the other. I direct that my attorney shall not be required to post a bond or to file with any Court or any public official any report or accounting relating to the administration of my affairs except to the extent that I have no power to excuse the filing of such reports or accounting. My said attorney shall furnish to me annually, or at more