

Question
Can anyone help me look at the form below to correctly identify the following: 1. entities identified in system 2. Attributes/fields of each entity, and
Can anyone help me look at the form below to correctly identify the following:
1. entities identified in system
2. Attributes/fields of each entity, and candidate keys (determinants)
3. Identify all possible functional dependencies
4. Create seperate entity to secure database (just a name)
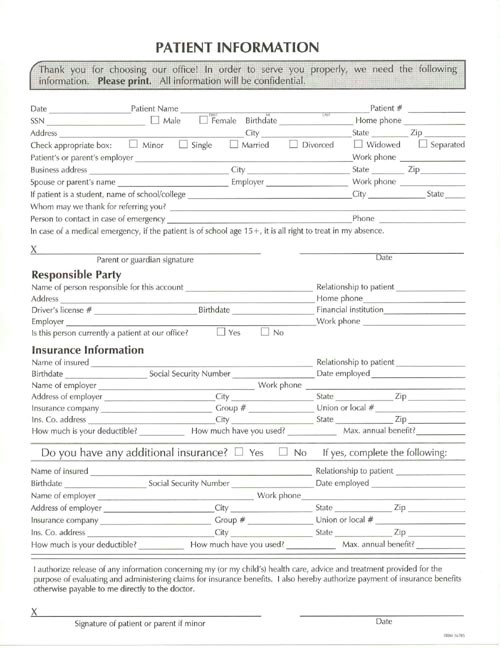
PATIENT INFORMATION Thank you for choosing our office! In order to serve you properly, we need the following information. Please print. All information will be confidential Date SSN atient Name Patient Home phone MaleFemale Bithdate City Check appropriate box:Minor Single Married Divorced Widowed Patient's or parent's employer Business address Spouse or parent's name If patient is a student, name of schoolcollege Whom may we thank for referring you Person to contact in case of emergency In case of a medical emergency, if the patient is of school age 15+, it is all right to treat in my absence Separated Work phone State Work phone State Parent or guardian signature Responsible Party Name of person responsible for this account Relationship to patient Home phone Financial institution Work phone Driver's license Is this person currently a patient at our office Insurance Information Name of insured Relationship to patient Date emplayed Social Security Number Work phone Name of employer Addeess of employer Insurance company Ins. Co. address How much is your deductibler State Union or local State Zip Group # City How much have you used? Max. annual benefit? No If Do you have any additional insurance? Sociall Security Number City City yes, complete the Relationship to patient Date employed Yes Name of insured Name of employer Address of employer Insurance company Ins. Co adkdress How much is your deductible? Work phone tate -Union or local # State How much have you used Max, annual benefit I authorize release of any information concerning my for my child's) health care, advice and treatment provided for the purpose of evaluating and administering caims for insurance benefts. also hereby authorize payment of insurance benefits ctherwise payable to me directly to the doctor Signature of patient or parent if minor PATIENT INFORMATION Thank you for choosing our office! In order to serve you properly, we need the following information. Please print. All information will be confidential Date SSN atient Name Patient Home phone MaleFemale Bithdate City Check appropriate box:Minor Single Married Divorced Widowed Patient's or parent's employer Business address Spouse or parent's name If patient is a student, name of schoolcollege Whom may we thank for referring you Person to contact in case of emergency In case of a medical emergency, if the patient is of school age 15+, it is all right to treat in my absence Separated Work phone State Work phone State Parent or guardian signature Responsible Party Name of person responsible for this account Relationship to patient Home phone Financial institution Work phone Driver's license Is this person currently a patient at our office Insurance Information Name of insured Relationship to patient Date emplayed Social Security Number Work phone Name of employer Addeess of employer Insurance company Ins. Co. address How much is your deductibler State Union or local State Zip Group # City How much have you used? Max. annual benefit? No If Do you have any additional insurance? Sociall Security Number City City yes, complete the Relationship to patient Date employed Yes Name of insured Name of employer Address of employer Insurance company Ins. Co adkdress How much is your deductible? Work phone tate -Union or local # State How much have you used Max, annual benefit I authorize release of any information concerning my for my child's) health care, advice and treatment provided for the purpose of evaluating and administering caims for insurance benefts. also hereby authorize payment of insurance benefits ctherwise payable to me directly to the doctor Signature of patient or parent if minor
Step by Step Solution
There are 3 Steps involved in it
Step: 1

Get Instant Access to Expert-Tailored Solutions
See step-by-step solutions with expert insights and AI powered tools for academic success
Step: 2

Step: 3
Ace Your Homework with AI
Get the answers you need in no time with our AI-driven, step-by-step assistance
Get Started
Deductive And Object Oriented Databases Third International Conference Dood 93 Phoenix Arizona Usa December 6 8 1993 Proceedings Lncs 760
Authors: Stefano Ceri ,Katsumi Tanaka ,Shalom Tsur
1993rd Edition
3540575308, 978-3540575306