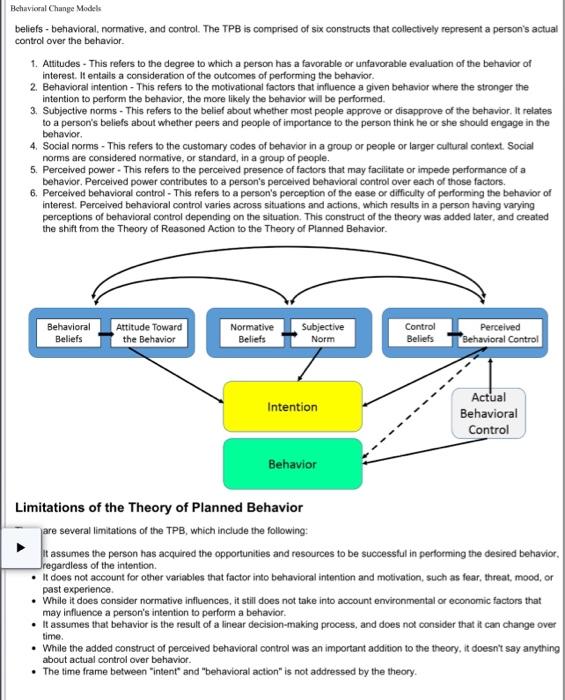
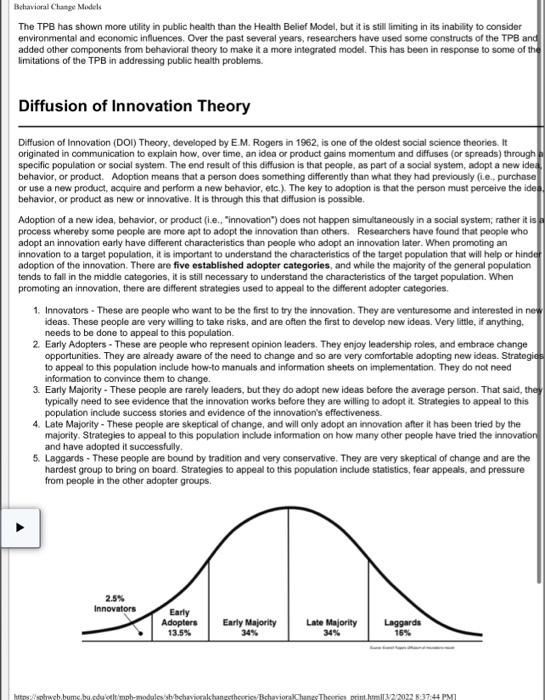
Case Study 3: The Health Belief Model and COVID- 19 Ar Using the Health Belief Model, discuss why some people might not have followed the "safer at home" practices (e.g., social distancing, masking, no large gatherings) after the vaccine became widely available. Minimum word count 250. ("Behavioral Change Models" discusses the Health Belief Model.) Public health is a multi-disciplinary field that aims to 1) prevent disease and death, 2) promote a better quality of ife, and 3) create environmental conditions in which people can be healthy by intervening at the institutional, community, and societal level. Whether public health practitioners can achieve this mission depends upon their abilty to accurately identify and define public health problems, assess the fundamental causes of these problems, determine populations most at-risk, develop and implement theory- and evidence-based interventions, and evaluate and refine those interventions to ensure that they are achieving their desired outcomes without unwanted negative consequences. To be effective in these endeavors, public health practitioners must know how to apply the basic principles, theories, research findings, and methods of the social and behavioral sciences to inform their efforts. A thorough understanding of theories used in public health, which are mainly derived from the social and behavioral sciences, allow practitioners to: - Assess the fundamental causes of a public health problem, and - Develop interventions to address those problems. Note: This module has been translated into Estonian by Marie Stetanova. The translation can be accessed at htips:/uww.bildeleekspert di/blog/2018/08/06/sotsiaalsete-normide-teooria/ Learning Objectives After successfully reviewing these modules, students will be able to: - List and describe the key constructs of the Health Belief Model and the theory of planned behavior and explain how they might be applied to develop effective public heath interventions - List and describe the elements of "perceived behavioral contror - Describe the underlying theory and basic elements of Social Norms Theory and marketing campaigns - List and describe the key constructs of Social Cognitive Theory and explain how they might be applied to develop effective public health interventions Summarize the criticisms that have been made regarding the major traditional models of health behavior change and why these models do not seem adequate to account for observed health behaviors Outine the major steps in the Transtheoretical Model - List the characteristics of each step of the Transtheoretical Model - Describe Diffusion of Innovation Theory and how it can be applied in heath promotion - Outline the basic structures of the Theory of Gender and Power and its application to Public Health - Explain the constructs of the Sexual Health Model and its application to public health The Health Belief Model The Heath Belief Model (HBM) was developed in the early 1950 s by social scientists at the U.S. Public Health Service in order to understand the failure of people to adopt disease prevention strategies or screening tests for the early detection of disease. Later uses of HBM were for patients' responses to symptoms and compliance with medical treatments. The HBM suggests that a person's belief in a personal threat of an illness or disease together with a person's belief in the effectiveness of the recommended health behavior or action will predict the likelihood the person will adopt the behavior. The HBM derives from psychological and behavioral theory with the foundation that the two components of health-related behavior are 1) the desire to avoid illness, or conversely get well if already ill; and, 2) the belief that a specific health action will Behavioral Change Models beliefs - behavioral, normative, and control. The TPB is comprised of six constructs that collectively represent a person's actual control over the behavior. 1. Attitudes - This refers to the degree to which a person has a favorable or unfavorable evaluation of the behavior of interest. It entails a consideration of the outcomes of performing the behavior. 2. Behavioral intention - This refers to the motivational factors that influence a given behavior where the stronger the intention to perform the behavior, the more likely the behavior will be performed. 3. Subjective norms - This refers to the belief about whether most people approve or disapprove of the behavior. It relates to a person's beliefs about whether peers and people of importance to the person think he or she should engage in the behavior. 4. Social norms - This refers to the customary codes of behavior in a group or people or larger cultural context. Social norms are considered normative, or standard, in a group of people. 5. Perceived power - This refers to the perceived presence of factors that may facilitate or impede performance of a behavior. Perceived power contributes to a person's perceived behavioral control over each of those factors. 6. Perceived behavioral control - This refers to a person's perception of the ease or difficulty of performing the behavior of interest. Perceived behavioral control varies across situations and actions, which results in a person having varying perceptions of behavioral control depending on the situation. This construct of the theory was added later, and created the shift from the Theory of Reasoned Action to the Theory of Planned Behavior. Limitations of the Theory of Planned Behavior are several limitations of the TPB, which include the following: it assumes the person has acquired the opportunities and resources to be successful in performing the desired behavior. regardless of the intention. - It does not account for other variables that factor into behavioral intention and motivation, such as fear, threat, mood, or past experience. - While it does consider normative inffuences, it still does not take into account emvironmental or economic factors that may influence a person's intention to perform a behavior. - It assumes that behavior is the result of a linear decision-making process, and does not consider that it can change over time. - While the added construct of perceived behavioral control was an important addition to the theory, it doesn't say anything about actual control over behavior. - The time frame between "intent" and "behavioral action" is not addressed by the theory. Bchavioral Chatpe Models The TPB has shown more utility in public health than the Health Belief Model, but it is still limiting in its inability to consider environmental and economic influences. Over the past several years, researchers have used some constructs of the TPB and added other components from behavioral theory to make it a more integrated model. This has been in response to some of the limitations of the TPB in addressing public health problems. Diffusion of Innovation Theory Diffusion of innovation (DOI) Theory, developed by E.M. Rogers in 1962, is one of the oldest social science theories. It originated in communication to explain how, over time, an idea or product gains momentum and diffuses (or spreads) through specific population or social system. The end result of this diffusion is that people, as part of a social system, adopt a new idea behavior, or product. Adoption means that a person does something differently than what they had previously (c.e., purchase or use a new product, acquire and perform a new behavior, etc.). The key to adoption is that the person must perceive the ide behavior, or product as new or innovative. It is through this that diffusion is possible. Adoption of a new idea, behavior, or product (i.e., "innovation") does not happen simultaneously in a social system; rather it is process whereby some people are more apt to adopt the innovation than others. Researchers have found that people who adopt an innovation early have different characteristics than people who adopt an innovation later. When promoting an innovation to a target population, it is important to understand the characteristics of the target population that will help or hinder adoption of the innovation. There are five established adopter categories, and while the majority of the general population tends to fall in the middle categories, it is still necessary to understand the characteristics of the target population. When promoting an innovation, there are different strategies used to appeal to the different adopter categories. 1. Innovators - These are people who want to be the first to try the innovation. They are venturesome and interested in ne? ideas. These people are very willing to take risks, and are often the first to develop new ideas. Very little, if anything. needs to be done to appeal to this population. 2. Early Adopters - These are people who represent opinion leaders. They enjoy leadership roles, and embrace change opportunities. They are already aware of the need to change and so are very comfortable adopting new ideas. Strategie: to appeal to this population include how-to manuals and information sheets on implementation. They do not need information to convince them to change. 3. Early Majority - These people are rarely leaders, but they do adopt new ideas before the average person. That said, the typically need to see evidence that the innovation works belore they are willing to adopt it. Strategies to appeal to this population include success stories and evidence of the innovation's effectiveness. 4. Late Majority - These people are skeptical of change, and will only adopt an innovation after it has been tried by the majority. Strategies to appeal to this population include information on how many other people have tried the innovation and have adopted it successfully. 5. Laggards - These people are bound by tradition and very conservative. They are very skeptical of change and are the hardest group to bring on board. Strategies to appeal to this population include statistics, fear appeals, and pressure from people in the other adopter groups. Source: httpilblog-leanmonitor.comlearly-adopters-allies-launching-product The stages by which a person adopts an innovation, and whereby diffusion is accomplished, include awareness of the need for an innovation, decision to adopt (or reject) the innovation, initial use of the innovation to test it, and continued use of the innovation. There are five main factors that influence adoption of an innovation, and each of these factors is at play to a different extent in the five adopter categories. 1. Relative Advantage - The degree to which an innovation is seen as better than the idea, program, or product it replaces. 2. Compatbility - How consistent the innovation is with the values, experiences, and needs of the potential adopters. 3. Complexity - How difficult the innovation is to understand and/or use. 4. Triability - The extent to which the innovation can be tested or experimented with before a commitment to adopt is made. 5. Observability - The extent to which the innovation provides tangible results. Limitations of Diffusion of Innovation Theory There are several limitations of Diffusion of Innovation Theory, which include the following: - Much of the evidence for this theory, including the adopter categories, did not originate in public health and it was not developed to explicitly apply to adoption of new behaviors or health innovations. - It does not foster a participatory approach to adoption of a public health program. - It works better with adoption of behaviors rather than cessation or prevention of behaviors. - It doesn't take into account an individuar's resources or social support to adopt the new behavior (or innovation). This theory has been used successfully in many fields including communication, agriculure, public health, criminal justice, social work, and marketing. In public health, Diffusion of Innovation Theory is used to accelerate the adoption of important public health programs that typically aim to change the behavior of a social system. For example, an intervention to address a public health problem is developed, and the intervention is promoted to people in a social system with the goal of adoption (based on Diffusion of innovation Theory). The most successful adoption of a public health program results from understanding the target population and the factors influencing their rate of adoption. For more on diffusion of innovation theory see "On the Diflusion of Innovations: How New ldeas Spread" by Leif Singer. The Social Cognitive Theory Social Cognitive Theory (SCT) started as the Social Learning Theory (SLT) in the 1960s by Abert Bandura. it developed into the SCT in 1986 and posits that learning occurs in a social context with a dynamic and reciprocal interaction of the person, environment, and behavior. The unique feature of SCT is the emphasis on social influence and its emphasis on external and intemal social reinforcement. SCT considers the unique way in which individuals acquire and maintain behavior. while also considering the social environment in which individuals perform the behavior. The theory takes into account a person's past experiences, which factor into whether behavioral action will occur. These past experiences influences reinforcements, evnertations, and expectancies, all of which shape whether a person will engage in a specific behavior and the reasons why a engages in that behavior. heories of behavior used in health promotion do not consider maintenance of behavior, but rather focus on initiating venavor. This is unfortunate as maintenance of behavior, and not just initiation of behavior, is the true goal in public health. The goal of SCT is to explain how people regulate their behavior through control and reinforcement to achieve goal-directed behavior that can be maintained over time. The first five constructs were developed as part of the SLT; the construct of selfefficacy was added when the theory evolved into SCT. 1. Reciprocal Determinism - This is the central concept of SCT. This refers to the dynamic and reciprocal interaction of person (individual with a set of leamed experiences), environment (external social context), and behavior (responses to stimuli to achieve goals). 2. Behavioral Capability - This refers to a person's actual ability to perform a behavior through essential knowledge and skills. In order to successfully perform a behavior, a person must know what to do and how to do it. People learn from the 1. Precontemplation - In this stage, people do not intend to take action in the foreseeable future (defined as within the next 6 months). People are often unaware that their behavior is problematic or produces negative consequences. People in this stage often underestimate the pros of changing behavior and place too much emphasis on the cons of changing bohavior. 2. Contemplation - In this stage, people are intending to start the healthy behavior in the foreseeable future (defined as within the next 6 months). People recognize that their behavior may be problematic, and a more thoughtful and practical consideration of the pros and cons of changing the behavior takes place, with equal emphasis placed on both. Even with this recognition, people may still feel ambivalent toward changing their behavior. 3. Preparation (Detemination) - In this stage, people are ready to take action within the next 30 days. People start to take small steps toward the behavior change, and they believe changing their behavior can lead to a healthier life. 4. Action - In this stage, people have recently changed their behavior (defined as within the last 6 months) and intend to keep moving forward with that behavior change. People may exhibi this by modifying their problem behavior or acquiring new healthy behaviors. 5. Maintenance - In this stage, people have sustained their behavior change for a while (defined as more than 6 months) and intend to maintain the behavior change going forward. People in this stage work to prevent relapse to earlier stages. 6. Termination - In this stage, people have no desire to return to their unhealthy behaviors and are sure they will not. relapse. Since this is rarely reached, and people tend to stay in the maintenance stage, this stage is often not considered in health promotion programs. ess through the stages of change, people apply cognitive, affective, and evaluative processes. Ten processes of have been identified with some processes being more relevant to a specific stage of change than other processes. processes result in strategies that help people make and maintain change. 1. Consciousness Raising - Increasing awareness about the healthy behavior. 2. Dramatic Relief - Emotional arousal about the health behavior, whether positive or negative arousal. 3. Self-Reevaluation - Self reappraisal to realize the healthy behavior is part of who they want to be. 4. Emvironmental Reevaluation - Social reappraisal to realize how their unhealthy behavior affects others. 5. Social Liberation - Environmental opportunities that exist to show society is supportive of the healthy behavior. 6. Self-Liberation - Commitment to change behavior based on the belief that achievement of the healthy behavior is possible. 7. Helping Relationships - Finding supportive relationships that encourage the desired change. 8. Counter-Conditioning - Substituting healthy behaviors and thoughts for unhealthy behaviors and thoughts. 9. Reinforcement Management - Rewarding the positive behavior and reducing the rewards that come from negative behavior