Cleveland Clinic: Transformation and Growth 2015 Mat we are undertaking would in many ways transform the world of medicine. Dr. Delos Cosgrove, CEO Cleveland Clinic
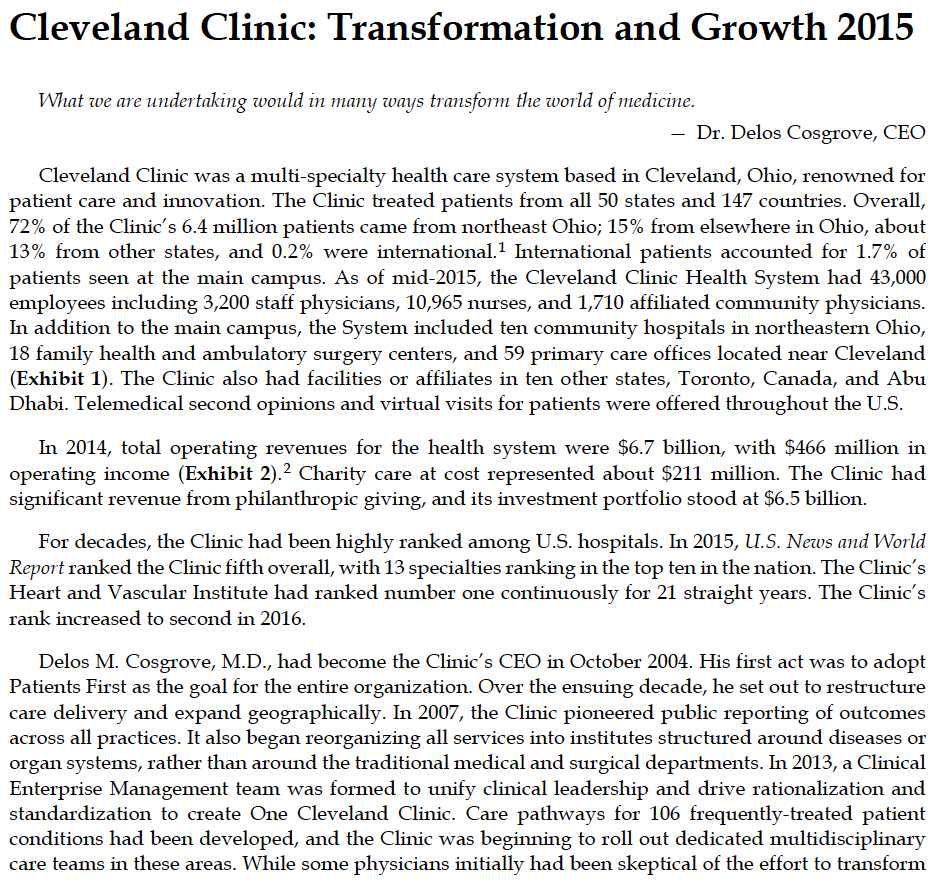
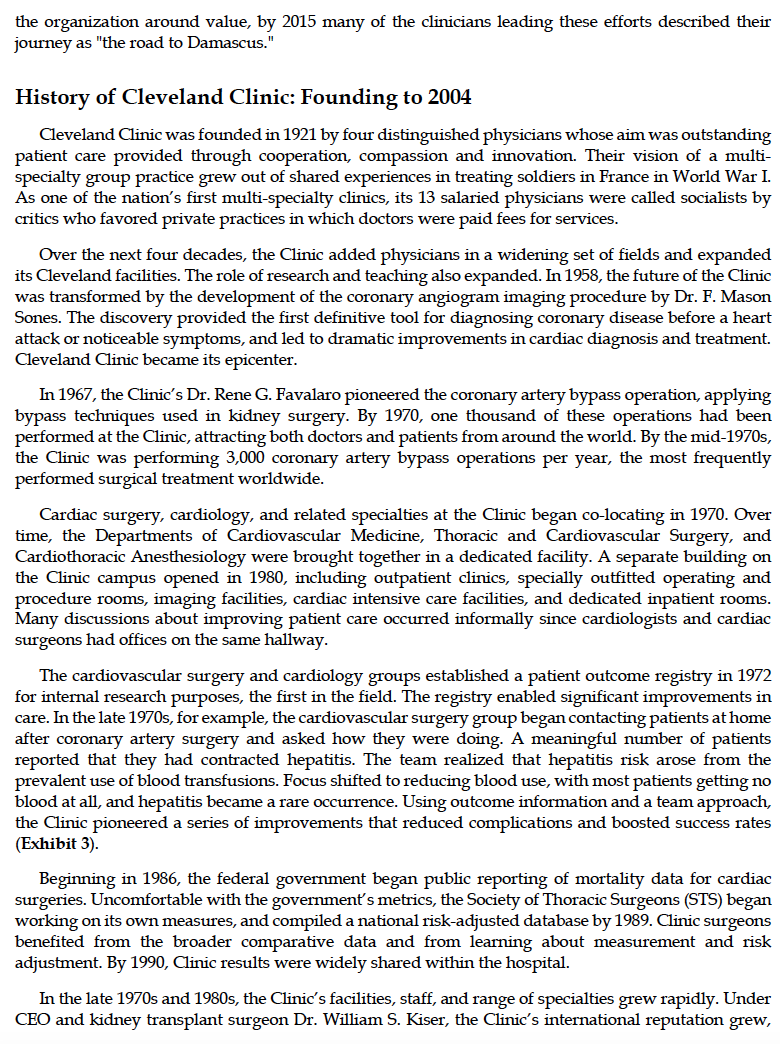
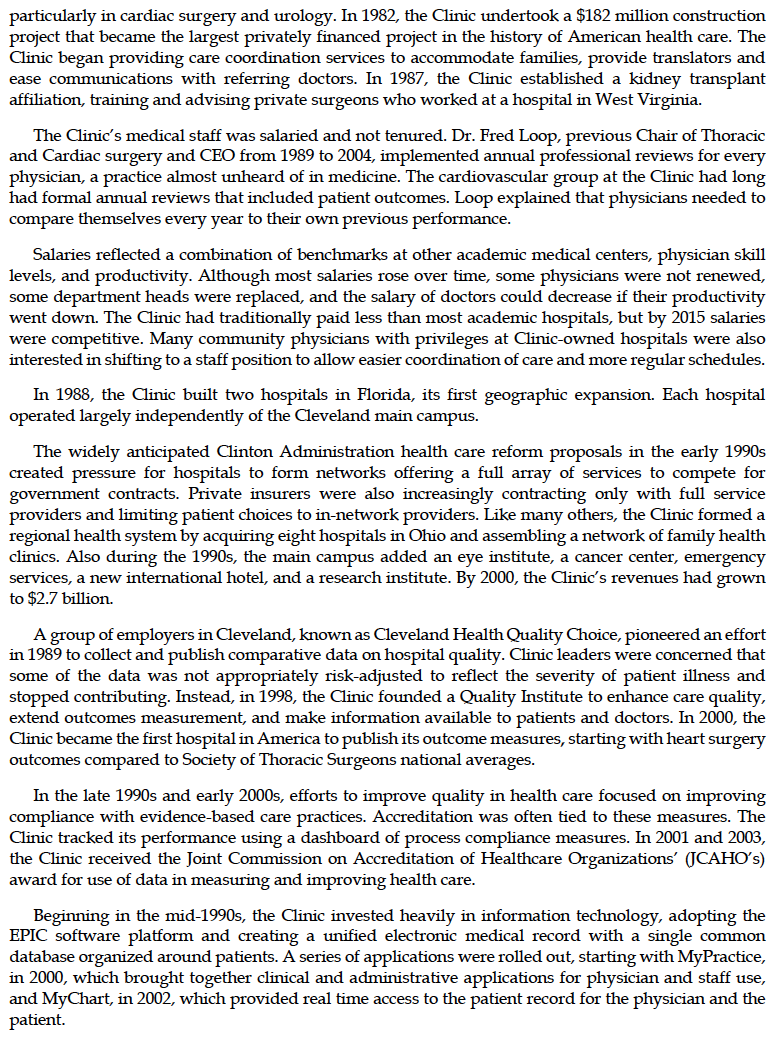
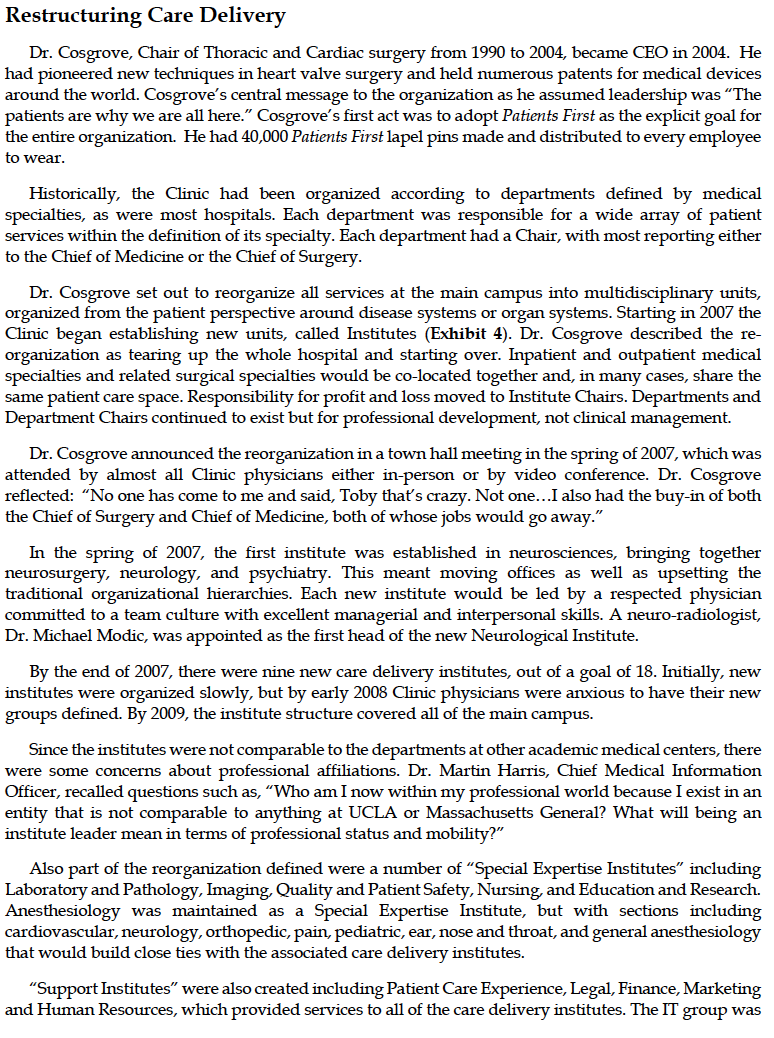
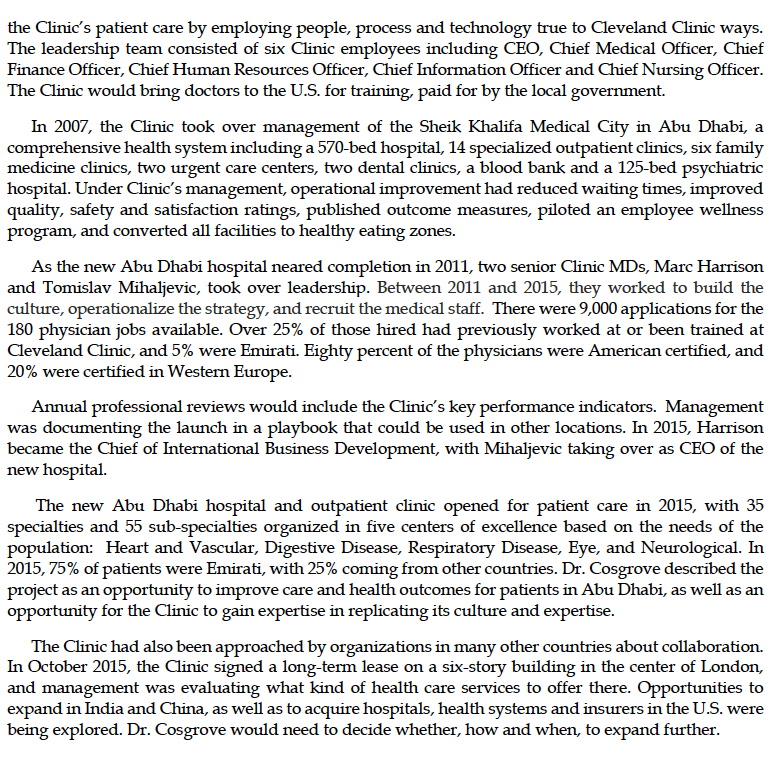
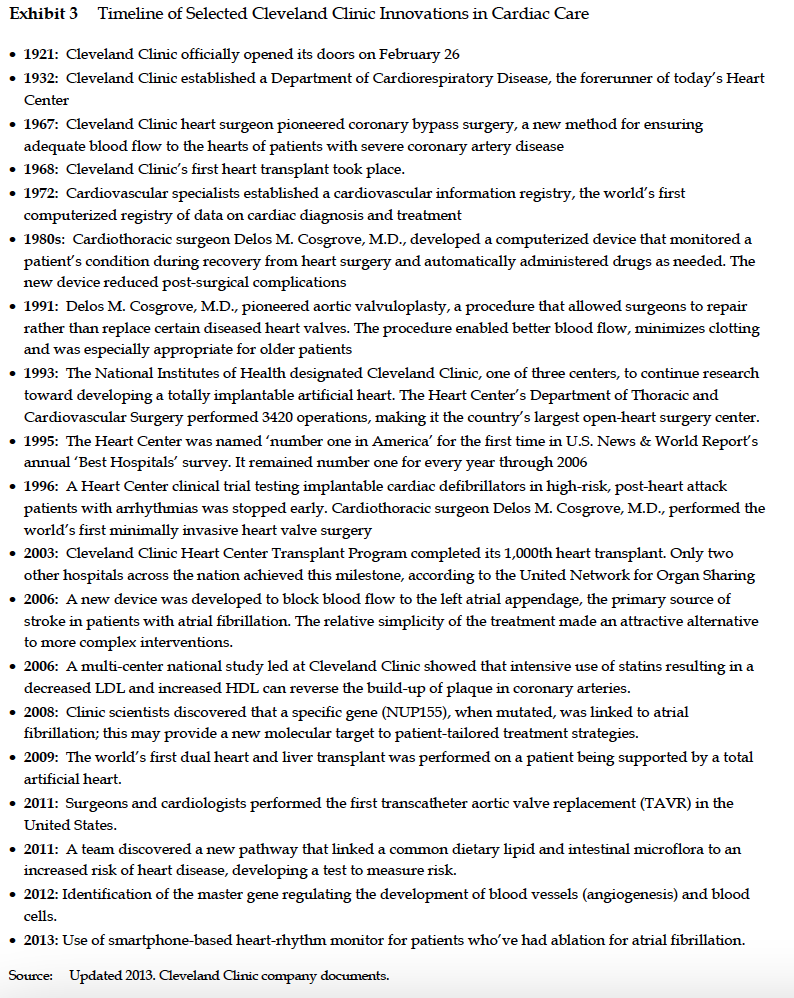
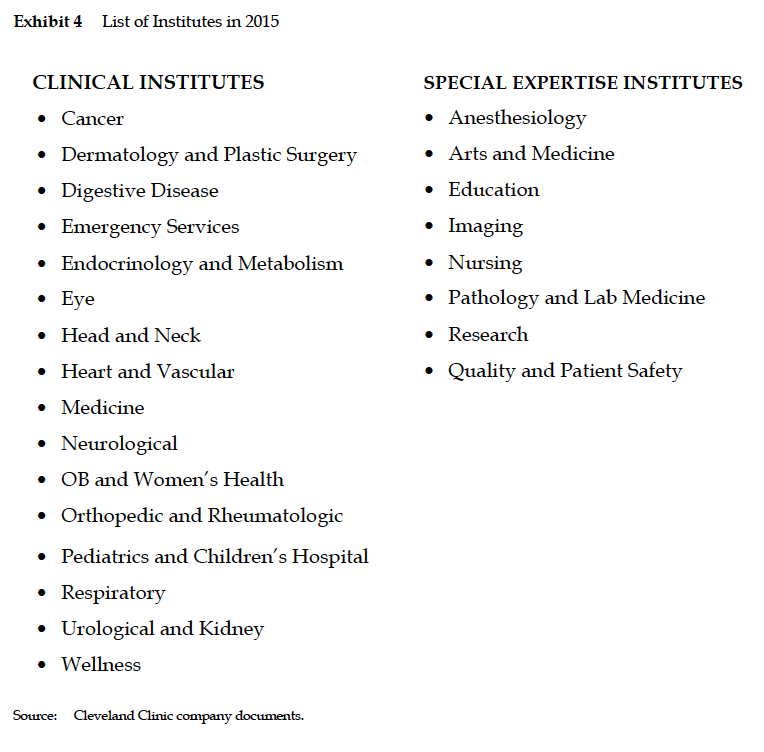
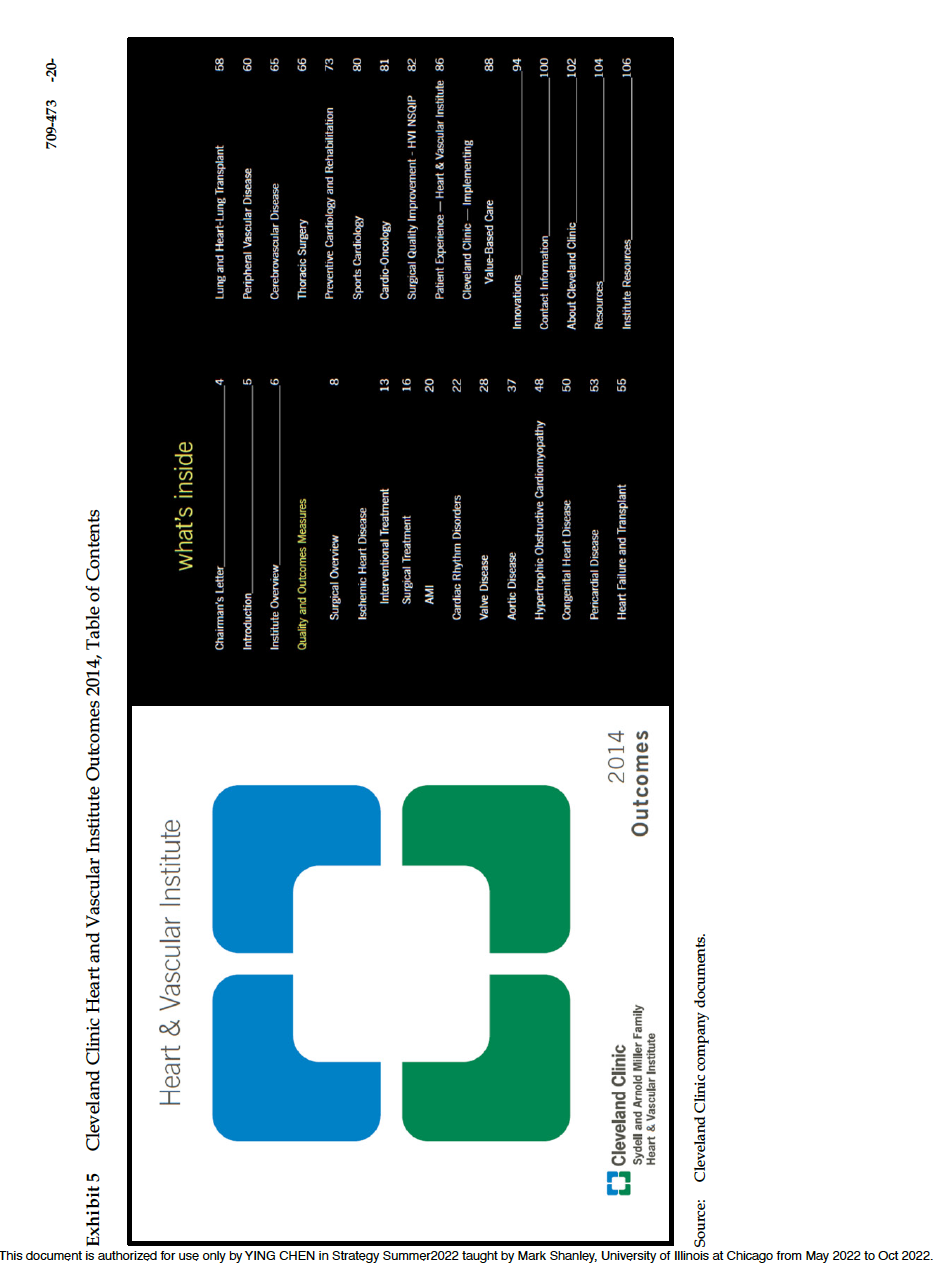
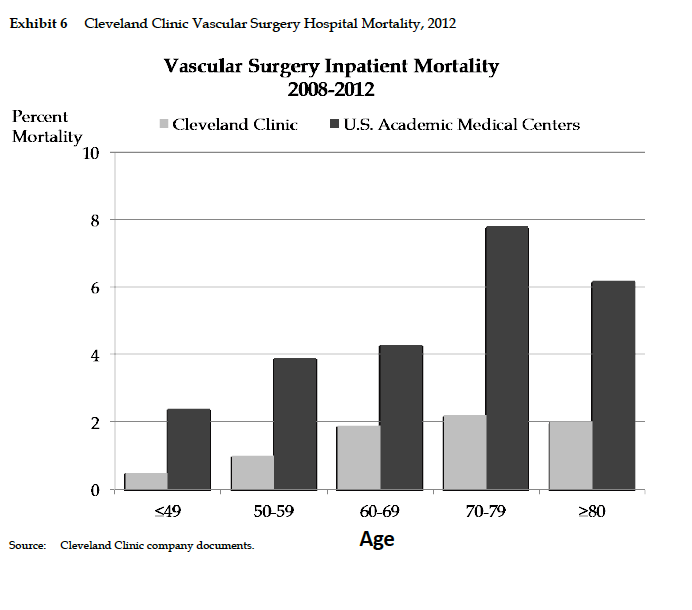
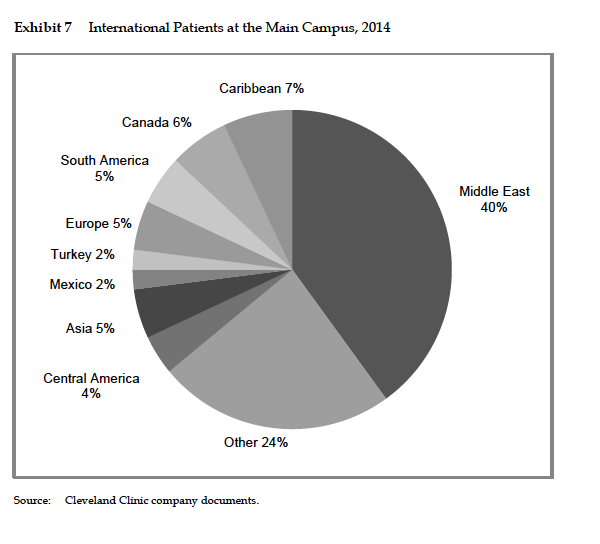
Cleveland Clinic: Transformation and Growth 2015 Mat we are undertaking would in many ways transform the world of medicine. Dr. Delos Cosgrove, CEO Cleveland Clinic was a multispecialty health care system based in Cleveland, Ohio, renowned for patient care and innovation. The Clinic treated patients from all 50 states and 147 countries. Overall, 72% of the Clinic's 6.4 million patients came from northeast Ohio,' 15% from elsewhere in Ohio, about 13% from other states, and 0.2% were international.1 International patients accounted for 1.7% of patients seen at the main campus. As of mid2015, the Cleveland Clinic Health System had 43,000 employees including 3,200 staff physicians, 10,965 nurses, and 1,710 affiliated community physicians. In addition to the main campus, the System included ten community hospitals in northeastern Ohio, 18 family health and ambulatory surgery centers, and 59 primary care offices located near Cleveland (Exhibit 1). The Clinic also had facilities or affiliates in ten other states, Toronto, Canada, and Abu Dhabi. Telemedical second opinions and virtual visits for patients were offered throughout the U.S. In 2014, total operating revenues for the health system were $6.7 billion, with $466 million in operating income (Exhibit 2).2 Charity care at cost represented about $211 million. The Clinic had significant revenue from philanthropic giving, and its investment portfolio stood at $6.5 billion. For decades, the Clinic had been highly ranked among US. hospitals. In 2015, [1.8. News and World Report ranked the Clinic fifth overall, with 13 specialties ranking in the top ten in the nation. The Clinic's Heart and Vascular Institute had ranked number one continuously for 21 straight years. The Clinic's rank increased to second in 2016. Delos M. Cosgrove, M.D., had become the Clinic's CEO in October 2004. His first act was to adopt Patients First as the goal for the entire organization. Over the ensuing decade, he set out to restructure care delivery and expand geographically. In 2007, the Clinic pioneered public reporting of outcomes across all practices. It also began reorganizing all services into institutes structured around diseases or organ systems, rather than around the traditional medical and surgical departments. In 2013, a Clinical Enterprise Management team was formed to unify clinical leadership and drive rationalization and standardization to create One Cleveland Clinic. Care pathways for 106 frequentlytreated patient conditions had been developed, and the Clinic was beginning to roll out dedicated multidisciplinary care teams in these areas. While some physicians initially had been skeptical of the effort to transform the organization around value, by 2015 many of the clinicians leading these efforts described their journey as "the road to Damascus." History of Cleveland Clinic: Founding to 2004 Cleveland Clinic was founded in 1921 by four distinguished physicians whose aim was outstanding patient care provided through cooperation, compassion and innovation. Their vision of a multi specialty group practice grew out of shared experiences in treating soldiers in France in World War I. As one of the nation' 5 rst multi specialty clinics, its 13 salaried physicians were called socialists by critics who favored private practices in which doctors were paid fees for services. Over the next four decades, the Clinic added physicians in a widening set of elds and expanded its Clevelandfacilities. Therole of researchand teaching also expanded. In 1953, the future ofthe Clinic was transformed by the development of the coronary angiogram imaging procedure by Dr. F. Mason Sones. The discovery provided the first definitive tool for diagnosing coronary disease before a heart attack or noticeable symptoms, and led to dramatic improvements in cardiac diagnosis and treatment. Cleveland Clinic became its epicenter. In 1967, the Clinic's Dr. Rene G. Favalaro pioneered the coronary artery bypass operation, applying bypass techniques used in kidney surgery. By 1970, one thousand of these operations had been performed at the Clinic, attracting both doctors and patients from around the world. By the mid19705, the Clinic was performing 3,000 coronary artery bypass operations per year, the most frequently performed surgical treatment worldwide. Cardiac surgery, cardiology, and related specialties at the Clinic began colocating in 1970. Over time, the Departments of Cardiovascular Medicine, Thoracic and Cardiovascular Surgery, and Cardiothoracic Anesthesiology were brought together in a dedicated facility. A separate building on the Clinic campus opened in 1980, including outpatient clinics, specially outfitted operating and procedure rooms, imaging facilities, cardiac intensive care facilities, and dedicated inpatient rooms. Many discussions about improving patient care occurred informally since cardiologists and cardiac surgeons had ofces on the same hallway. The cardiovascular surgery and cardiology groups established a patient outcome registry in 1972 for internal research purposes, the rst in the eld. The registry enabled signicant improvements in care. In the late 19705, for example, the cardiovascular surgery group began contacting patients athnme aftetcoronaryartetysurgeryandaskedhowtheyweredoing. Ameaningfulmimbercfpatients reported that they had contracted hepatitis. The team realized that hepatitis risk arose from the prevalent use of blood transfusions. Focus shifted to reducing blood use, with most patients getting no blood at all, and hepatitis became a rare occurrence. Using outcome information and a team approach, the Clinic pioneered a series of improvements that reduced complications and boosted success rates (Exhibit 3). Beginning in 1986, the federal government began public reporting of mortality data for cardiac surgeries. Uncomfortable with the government' 5 metrics, the Society of Thoracic Surgeons (ST'S) began working on its own measures, and compiled a national riskadjusted database by 1989. Clinic surgeons benefited from the broader comparative data and from learning about measurement and risk adjustment. By 1990, Clinic results were widely shared within the hospital. In the late 19705 and 1980s, the Clinic's facilities, staff, and range of specialties grew rapidly. Under CEO and kidney transplant surgeon Dr. William S. Kiser, the Clinic's international reputation grew, particularly in cardiac surgery and urology. In 1982, the Clinic undertook a $182 million construction project that became the largest privately nanced project in the histctry of American health care. The Clinic began providing care coordination services to accommodate families, provide translators and ease communications with referring doctors. In 1987, the Clinic established a kidney transplant affiliation, training and advising private surgeons who worked at a hospital in West Virginia. The Clinic's medical staff was salaried and not tenured. Dr. Fred Loop, previous Chair of Thoracic and Cardiac surgery and CEO from 1989 to 2004, implemented annual professional reviews for every physician, a practice almost unheard of in medicine. The cardiovascular group at the Clinic had long had formal annual reviews that included patient outcomes. Loop explained that physicians needed to compare themselves every year to their own previous performance. Salaries reflected a combination of benchmarks at other academic medical centers, physician skill levels, and productivity. Although most salaries rose over time, some physicians were not renewed, some department heads were replaced, and the salary of doctors could decrease if their productivity went down. The Clinic had traditionally paid less than most academic hospitals, but by 2015 salaries were competitive. Many community physicians with privileges at Clinicowned hospitals were also interested in shifting to a staff position to allow easier coordination of care and more regular schedules. In 1988, the Clinic built two hospitals in Florida, its first geographic expansion. Each hospital operated largely independently of the Cleveland main campus. The widely anticipated Clinton Administration health care reform proposals in the early 1990s created pressure for hospitals to form networks offering a full array of services to compete for government contracts. Private insurers were also increasingly contracting only with full service providers and limiting patient choices to innetwork providers. Like many others, the Clinic formed a regional health system by acquiring eight hospitals in Ohio and assembling a network of family health clinics. Also during the 19905, the main campus added an eye institute, a cancer center, emergency services, a new international hotel, and a research institute. By 2000, the Clinic's revenues had grown to $2.7 billion. A group of employers in Cleveland. known as Cleveland Health Quality Choice, pioneered an effort in 1989 to collect and publish comparative data on hospital quality. Clinic leaders were concerned that some of the data was not appropriato riskadjusted to reect the severity of patient illness and stopped contributing. Instead, in 1998, the Clinic founded a Quality Institute to enhance care quality, extend outacornes measurement, and make information available to patients and doctors. In 2000, the Clinic became the first hospital in America to publish its outcome measures, starting with heart surgery outcomes compared to Society of Thoracic Surgeons national averages. In the late 19905 and early 20005, efforts to improve quality in health care focused on improving compliance with evidencebased care practices. Accreditation was often tied to these measures. The Clinic tracked its performance using a dashboard of process compliance measures. In 2001 and 2003, the Clinic received the Ioint Commission on Accreditation of Healthcare Organizations' (ICAHO's) award for use of data in measuring and improving health care. Beginning in the mid1990s, the Clinic invested heavily in information technology, adopting the EPIC software platform and creating a unified electronic medical record with a single common database organized around patients. A series of applications were rolled out, starting with MyPractice, in 2000, which brought together clinical and administrative applications for physician and staff use, and MyChart, in 2002, which provided real time access to the patient record for the physician and the patient. Restructuring Care Delivery Dr. Cosgrove, Chair of Thoracic and Cardiac surgery from 1990 to 2004, became CEO in 2004. He had pioneered new techniques inheart valve surgery and held numerous patents for medical devices around the world. Cosgrove's central message to the organization as he assumed leadership was "The patients are why we are all here.\" Cosgrove's rst act was to adopt Patients First as the explicit goal for the entire organization. He had 40,000 Patients First lapel pins made and distributed to every employee to wear. Historically, the Clinic had been organized according to departments defined by medical specialties, as were most hospitals. Each department was responsible for a wide array of patient services within the definition of its specialty. Each department had a Chair, with most reporting either totheChiefofMeditineortheChiefofSurgery. Dr. Cosgrove set out to reorganize all services at the main. campus into multidisciplinary units, organized from the patient perspective around disease systems or organ systems. Starting in 2007 the Clinic began establishing new units, called Institutes {Exhibit 4). Dr. Cosgrove described the re organization as tearing up the whole hospital and starting over. Inpatient and outpatient medical specialties and related surgical specialties would be colocated together and, in many cases, share the same patient care space. Responsibility for profit and loss moved to Institute Chairs. Departments and Department Chairs conrmed to exist but for professional development, not clinical management. Dr. Cosgrove announced the reorganization in a town hall meeting in the spring of 2007, which was attended by almost all Clinic physicians either inperson or by video conference. Dr. Cosgrove reected: "No one has come to me and said, Toby that's crazy. Not one...l also had the buyin ofboth the Chief of Surgery and Chief of Medicine, both of whose jobs would go away." In the spring of 2007, the rst institute was established in neurosciences, bringing together neurosurgery, neurology, and psychiatry. This meant moving offices as well as upsetting the traditional organizational hierarchies. Each new institute would be led by a respected physician committed to a team culture with excellent managerial and interpersonal skills. A neuroradiologist, Dr. Michael Modic, was appointed as the first head of the new Neurological Institute. By the end of 2007, there were nine new care delivery institutes, out of a goal of 18. Initially, new institutes were organized slowly, but by early 2008 Clinic physicians were anxious to have their new groups dened. By 2009, the institute structure covered all of the main campus. Since the institutes were not comparable to the departments at other academic medical centers, there were some concerns about professional affiliations. Dr. Niartin Harris, Chief Medical Information Ofcer, recalled questions such as, "Who am I now within my professional world because I exist in an entity that is not comparable to anything at UCLA or Massachusetts General? What will being an institute leader mean in terms of professional status and mobility. " Also part of the reorganization defined were a number of "Special Expertise Institutes" including Laboratory and Pathology, Imaging, Quality and Patient Safety, Nursing, and Education and Research. Anesthesiology was maintained as a Special Expertise Institute, but with sections including cardiovascular, neurology, orthopedic, pain, pediatric, ear, nose and throat, and general anesthesiology that would build close ties with the associated care delivery institutes. \"Support Institutes\" were also created including Patient Care Experience, Legal, Finance, Marketing and Human Resources, which provided services to all of the care delivery institutes. The IT group was reorganized to assign IT personnel to every clinical and special expertise institute. As part of the reorganization, the Clinic added two positions that rarely existed in other hospital systems: a Chief Wellness Ofcer (2005) and a Chief Experience Ofcer {2007]. Institute leadership teams had to dene what diseases and conditions the institute cared for, develop a set of shared outcome measures for which the team would be jointly accountable, and identify the skills that needed to be brought together to care for patients including consultative services such as psychiatry. Since institute physicians would generate revenues together, rather than as individuals, traditional differences in compensation would not necessarily persist. One physician described the new reorganization as "akin to mixing matter with antimatter, but the process is somewhat easier." Across the institutes, clinical transformation efforts were uneven. Some institutes, such as Neurosciences and Heart and Vascular, moved rapidly to organize services around patient conditions. The Neurological Institute organized 10 multidisciplinary centers for conditions such as epilepsy, brain tumors, sleep disorders, neurological restoration, and multiple sclerosis. In many other Institutes, however, there were limited changes to care delivery other than colocation. In 2012, Dr. Cosgrove created the position of Chief Strategy Ofcer to work with Clinic leadership in setting the future direction of the organization, naming Ann Huston, a leader in Ernst & Young's national health care strategy practice. Huston and Dr. David Longworth, Chair of the Medicine Institute, led a process to dene the next stage of the transformation to patient value, the core principle of the enterprise strategy. The Cleveland Clinic Integrated Care Model (CCICM), a patientcentered, valuebased model of care was the centerpiece. The CCICM aimed to create a seamless experience for patients as they received care over time and across different Clinic and nonClinic sites. Integration would be the responsibility of the provider. Through a series of weekly meetings the leadership team began clinical transformation projects to improve outconres, efciency and patient experience. Specied care paths were developed, starting with less complex conditions where the Clinic had high volume, performance gaps or financial exposure, and where there were publicly reported outcome measures or opportunities such as new payment model initiatives. By late 2014, care paths had been identied for 106 conditions. Some were wholly within an Institute, while some included team members from other institutes to cover the care cycle. Inback pain, for example, the team focused on ways to avoid unnecessary interventions, utilize lower cost providers, or offer alternative care approaches. In this condition alone, cost savings had already reached $1.9 million per year. In obstetrics, the team found opportunities to reduce unnecessary induction of labor and frequency of Csections. Neurosciences had long been a leader. By 2014, Neurosciences had 12 condition units and was dening outcome measures and improved care approaches for each For example, the multidisciplinary stroke team analyzed the effectiveness of MRI to determine which patients could benet from endovascular treatments to restore blood ow to the brain, and improvement in the effectiveness of use of drugs to dissolve blood clots. Patients' functional outcomes improved and risk adjusted costs fell by almost 25%. In December 2014, Dr. Cosgrove named Dr. Modic to the new position of Chief Clinical Transformation Ofcer, and Dr. Brian Donley to Chief of Clinical Enterprise and Chief of Staff. Donley had been the president of all of the regional hospitals, andbefore that the CEO of Lutheran Hospital, a community hospital in the System Clinic least envisioned an evolution towards structuring most of Clinic services in multi disciplinary teams based on the logic of how a patient moved through the care continuum. In the new model, a physician or other caregiver could be a member of multiple care teams, but every team would have consistent members who worked together regularly and measured results. In 2015, implementation in Institutes was underway. Four integrated practice units were created for breast cancer, colorectal cancer, back pain and mitral valve disease. New outcomes measures and patient experience measures were being rolled out. A learning collaborative was created among the four EPUs to overcome obstacles and develop insights that would accelerate the change process for future teams. As of 2015, the network of conrmunity hospitals continued to operate using the traditional departmental structure, thoughintegrating them into institute care paths and results measurement was underway. The Clinic was also working to connect care with community based primary care practices as well as postacute care, skilled musing facilities, rehabilitation, and home care to offer a fully integrated care experience. This CCICIH would be the basis of the Clinic's population health initiatives. Measurement Dr. Cosgrove's central message, Patients First, demanded relentless focus on measurable quality by improving structure, processes and outcomes. This included respectfor the patient's dignity, excellence in housekeeping services and facilities, and genuine concern for the patient's emotional wellbeing and care experience. Dr. Cosgrove saw patient outcomes as "the ultimate measure of quality.\" In 2005, shortly after becoming CEO,heaskedalldepartmentsto measuretheirhealthoutccmesandpreparetoreport outcomes publicly in print and on the web. Every clinical team would need to consider carefully what it meant to improve the health of its patients. Since surgeons were more accustomed to outcomes measurement, the surgery groups were asked to begin public reporting in one year and the medical groups in two years. By 2007, the Clinic published outcome books for every department, comparing itself to the best available benchmarks {Exhibits 5 and 6 give excerpts].5 Outcome measurement differed in sophistication across groups. When a department reported process metrics or the numbers of procedures or patients served, rather than patient health outcomes, Dr. Cosgrove would thank them, explain that he had committed to publicly reporting health outcomes of patients, and ask the team to work on that for the next report. The Clinic saw the core purpose of measuring outcomes as enabling learning and quality improvement by teams, rather than for the sake of obtaining referrals, marketing, or boosting national ratings. The primary external audience was peer physicians. The secondary purpose, after driving improvement in outcomes, was transparency. Dr. Ccsgrove explained, "We can't be best at everything. The more you put out there, the more credibility you have. In doing so, we challenge others to do the same. We can learn from others who maybe performing better thanwe are." When the Clinic reorganized into Institutes, each Institute was charged with deciding what dened good care for their patients' conditions, rather than for procedures. In 2015, some outconre books were still largely based on volume and process measures required by payers, and there was uncertainty about how outcomes should be measured and reported. Progress was being driven by the care path and integrated practice unit: initiatives, as well as by the Knowledge Program (KP) which collected patientreported outcomes and health status measures on tablets at each appointment and put them directly in the electronic health record. By 2015, KP data on cognition, mood, social and functional outcome measures had been collected in hundreds of thousands of encounters, mostly for patients with epilepsy, sleep disorders, inflammatory bowel and stroke. On costs, as with most hospitals, charges and costs were measured by procedure or by hospital day. In 2006, Steve Glass, CFO, launched a major effort to understand costs over the cycle of care for specic service lines. Legacy accounting systems at different Clinic hospitals often assigned different costs to the same activities or supplies. Glass worked to justify those differences or eliminate them. He also worked to understand the actual array of activities thatwenf into care of eachmedical condition over its full care cycle rather than just analyze charges. As awareness increased on deficiencies in hospital costing practices, the Clinic engaged in pilots to compare the different costing approaches. The initiatives to develop care paths and map the activities in the patient care continuum would enable improvement in costing. Steps were taken to improve transparency about costs, starting with supplies. Most physicians had previously been unaware of what supplies cost. One group discovered items in the surgical pack that were never used, though each surgeon had assumed they were useful to someone else. Another group discovered that it could reduce costs of surgical materials without affecting outcomes if surgeons closed surgical sites with a $5 silk suture instead of using $400 staples. The use of surgical staplers dropped from 91% to 10%. Other groups used cost and quality evidence to standardized supplies. In 2013 the Clinic created Excelerate, a providerled joint venture with VI-IA to reduce costs in purchasing. A special focus was to address physician preference items which could increase physicianhospital alignment. In its first year of participation in Excelerate, Akron General realized $4 million in savings. In 2013, Cosgrove set out to reduce costs by $1.5 billion over the next five years to address cost pressures and adapt to declining reimbursement by both public and private payers. The Clinic created the Care Affordability task force to study its administrative and clinical costs with consulting firm support and benchmarking of other hospitals. Steps included consolidating preadmissions testing and imaging, sharing staff across sites, eliminating about 1600 FTEs over 2 years, and hundreds of other changes. Dr. Cosgrove explained that everyone at the Clinic bought in, though the process was painstaking. By July 2015 resulting cost reductions had totaled $513 million ($171 million in indirect administrative costs; $275 million in clinical costs, $60 million in regional hospital costs, and $7 nrillion of other including research and education). Indirect costs had fallen by 16%, and clinical costs by 9%. An additional $100 million of cost reductions was already planned for 2016 and 2017. Wellness Beginning in 2005, the Clinic signicantly increased its focus on wellness, starting with its own employees who were covered by a selfinsured health plan at an annual cost of $250 million. Smoking cessation was the first major initiative. In 2006, the Clinic supported successful ballot initiatives to ban smoking in public places in Ohio. Unspent money committed to that campaign was used to offer free smoking cessation classes to everyone in Cuyahoga County (the Clinic's home] for six months in 2006. The county achieved twice the cessation rate of the rest of Ohio. The Clinic also announced that it would no longer hire smokers and offered smoking cessation classes to any employee who needed thenL By 2007, the Clinic had become a smoke-free environment, and Cuyahoga County had gone from having the highest incidence of smokers in the state to the lowest. By 2008, a third of employees had participated inhealth Iisk appraisals (ERAS) and programs aimed at behavior change were helping people to lose weight, quit smoking, better manage stress, improve eating habits, and increase physical activity. [112012, the Clinic had moved away from HRAs in favor of asking employees to see their Cleveland Clinic primary care provider, who would assess risks and guide appropriate health management. Participating employees could get premium rebates on their health insurance if they met targeted goals. Employees with obesity, hypertension, smoking, or diabetes could get free coaching and support through the Clinic's disease management programs, which had a 57% participation rate in 2014. Between 2010 and 2015, annual growth in the Clinic's employee health care cost had fallen to 2.8%, down from 7.5% between 2004 to 2W9. The Clinic had achieved reductions in inpatient admissions for patients with chronic disease and reduced use of imaging and the emergency room. Leaders viewed employee health improvements as a test bed for managing future population health and accountable care contracts. Patient Experience In 2007, Cleveland Clinic became the rst health care organization to appoint a Chief Experience Ofcer or CXO. While outcomes were the ultimate measure of success, patient perceptions were strongly affected by the care experience. Dr. Cosgrove often observed that \"patients don't care how much we know, until they know how much we care." Efforts began by encouraging doctors and nurses to askpatients, "W'hatelsecanwe doforyouwhileyouarehere?"Thisincreasedfocusons ' care needs, anxiety, or depression and alerted staff to issues about food or the room Among the new services introduced were more and quieter single occupancy rooms, with pullout beds on which family members could sleep, unrestricted visiting hours and redesigned gowns that resembled bathrobes to protect the patient' 5 dignity. Clinic leaders wanted to instill a culture of service, where everyone was responsible for the patient experience. Beginning in 2007, the Clinic annually surveyed all employees to assess their commitment and connection to the Clinic' 5 purpose. The resulting employee engagement scores were compared to other organizations. Managers developed action plans to improve engagement, and included engagement scores in the animal reviews of managers. Overall Caregiver engagement relative to other organizations rose from the 44\"1 percentile in 2008 to the 37m percentile in 2013.4 Clinic leaders worked to make the concept of patient experience much more than hospitality. Experience was viewed as a measurable performance metric like clinical outcomes. The Clinic learned that when nurses rounded hourly, patient experience metrics were in the 90\"1 percentile or above, so hourly rounding was mandated for all Clinic hospitals. The work to improve care coordination and patient transitions encouraged managers to think beyond the processes in their direct control and explicitly consider how the patient experiences the continuum of care. Traditionally, nonphysicians at Cleveland Clinic had been designated as "nonprofessional staff\" whether they were nurses, technicians, therapists, janitors, or IT experts. In 2010, Dr. Cosgrove changed the designation of all employees to Caregivers. Employees, including physicians, engaged infacilitated smallgroup discussions about the mission, vision, values, patient experience and service standards of the Clinic. By 2014, patient satisfaction had improved and patient complaints dropped measurably. Another new practice was Leadership Rounding. In groups of two or three, 160 Clinic leaders each month talked with nurses and patients using a checklist of questions, and met afterwards to set action items. In 2012, the Clinic began offering same day appcdntments when needed. Clinic leaders realized that some urgent calls were coming in as appointment requests, and that for many people there was significant stress in waiting. In the new approach, the scheduler let the patient know same day appointments were available and helped the patient determine if they needed one. Operationally, this turned out to have advantages in utilizing younger staff, whose schedules might not otherwise be full, though some concerns were raised about the inefciency of patients not seeing the most appropriate Clinician for their situation Starting in 2012, the Clinic designed and delivered communications workshops for all employed physicians, fellows, residents, and marry afliated physicians and executives. These had the goal of improving relationships between physicians and patients, and among the caregivers. The Clinic used its own formula to track patient satisfaction data. The ratings were measurably higher for physicians after the communication workshops.5 Health System Rationalization The Clinic's Ohio hospital and outpatient network consisted of three larger hospitals located on the east, west and south sides of greater Cleveland and seven smaller community hospitals. Akron General, acquired in 2015, was the largest with almost 900 physicians and $600 million in operating revenues in 2014. The 140 employed physicians were employed in a traditional physician employment model and Akron's 700 nurses were unionized. Overall, admitting physicians at the comrnurlity hospitals were 45% Clinic staff physicians and 55% physicians in private practice. Six of the hospitals were profitable, while others registered modest losses. In total, the community hospitals had 1.7 times the admissions of the main hospital and one third of the revenue. Patient satisfaction at all of the community hospitals remained below that of the main C flinic facility. The goal going forward was defined as One Cleveland Clinic. Obstetrics was moved almost exclusively to community hospitals. Some community facilities concentrated on outpatient services and urgent care. Inpatient psychiatry services were concentrated into one community hospital location, and rehabilitation into two facilities. The number of trauma centers was reduced from 5 to 3 and Cleveland Clinic was a founding member of the northern Ohio trauma system that worked with emergency medical services to coordinate patient triage. Neurosurgery practices on the east side of Cuyahoga county were integrated into a common coordinated team that quickly evaluated patients locally and treated or coordinated transfer and treatment at the best suited facility. Other services, such as orthopedic surgery, were relocated (though not exclusively] from the main campus to other system hospitals. On the maincampus, three vascular labs were combined, as were three pulmonary care units. A community hospital near the main campus in central Cleveland was closed in 2011 and replaced with an outpatient center for chronic disease and services for atrisk teens. Conversion to outpatient facilities was also planned for Lakewood community hospital, owned by the city in which it was located and operated by the Clinic. Over time, efforts were made to coordinate care more tightly across locations. The goal was to have multispecialty teams use systemwide resources to deliver the right care at the right place for every patient, at the right time at the right cost. Community hospitals referred patients needing quaternary care, or the most complicated and acute care, to the main campus. In 2014, the postacute rehabilitation for stroke and other neurology patients had been included in the responsibilities and outcome measurement of the Neurological Institute. Modic explained that incorporating rehabilitation, home care and hospice services enabled the team to develop insights about improving patient outcomes over a fuller care cycle. To better integrate the network, the goal was to have a common electronic medical record, conmlon outcomes reporting, and unied medical staff planning and purchasing. For the rst time ever, in September 2010, the boards of all of the comnuinity hospitals met together at a retreat to create one standard for quality, patient safety and patient experience. Each hospital conrmed to have local management and accountability, but with the same administrative structure, standardized annual quality reporting and measurement, and common managerial systems. All hospitals had been reporting process, safety and satisfaction metrics, though the variability of the scores on these metrics among facilities was still wider than Clinic leaders desired. In 2015, the Clinic became a founding member of the Ldwest Health Collaborative, an alliance among six Ohiobased health systems encompassing about onethird of Ohio's inpatient activity. Members included ProMedica (Toledo), Aultman (Carlton), OhioI-Iealth (Columbus), Premier Health Partners (Dayton), and TriHealth (Cincinnati). This collaborative was working to develop statewide contracts with the state government and with employers as well as to build a shared clinical transformation platform to mitigate the overhead costs for new services. The first initiatives were analyzing data from all of the health systems to find the best approaches and most costeffective supplies for specic conditions. The initial areas of focus were on readmissions, diabetes, high risk maternity care, and low back pain. Information Technology The Cleveland Clinic was an early adopter of the EPIC health IT system, implementing it in 2001, five to ten years ahead of many large hospital systems. In 2015, the Clinic had a unified integrated electronic medical record system, MyPractice, serving all Cleveland Clinic physicians. Using a single common data warehouse, the system was organized longitudinally by patient. All applications, whether they were clinical, administrative or financial, were views of this database. The Clinic's system used the most robust and accepted information standards available for each type of record.'5 Patient records included digital data and images, test values, doctors' reports, and extracted values from non digital data such as echocardiograms. When possible, lab computers and medical devices transmitted data directly to the database. From this platform, MyChart enabled the physician and the patient to access the same information"? Patients could see records, request and cancel appointments, request prescription renewals, and notify the doctors about changes to mail or email addresses. For referring physicians, the Clinic introduced Dr.Connect in 2005. A secure, realtime pctrtal where physicians could review the care being delivered to their patients, Dr.Connect allowed referring physicians to access the records of their patients in real time. Electronic prescribing was also introduced, as was MyPractice Community which enabled doctors not affiliated with Cleveland Clinic to purchase the software addon for a monthly fee and communicate with other providers in the system MyPractice Community came prepopulated with patient data from all previous encounters within Cleveland Clinic health system and was able to transmit prescription and laboratory orders electronically, collect key process and outcome measures, and share clinical information across the Cleveland Clinic systenL As comrrtunity doctors became part of the Clinic's institutes, use of the Clinic's electronic medical record helped to improve coordination with Institutes' care processes. Dr. Martin Harris had led the effort to enable information technology to support outcome measurement, learning, and improvement by multidisciplinary teams. Institute teams were defining cycles of care for patients with particular conditions, and the IT group was developing support tools foreachtype ofpatientencounterinthecare cycle. Dr.Harrisemphasizedthatthegoalofthiscustom development was to efficiently support each institute's particular care processes and spur realtime knowledge generation and dissemination across the system. MyChart, the patient portal, was redesigned to encourage enrollment when a patient made an appointment. If a patient signed up, he or she could immediately manage registration information, worker's compensation forms, or special insurance considerations for their condition In addition, conditionspecific questionnaires were developed within the institutes that would replace general medicalhistoryformsandfeed directlyinto thepatient'schart. The chartwould thenbe sentto the physician's inbox for review before a patient' 5 visit. Explorrys, owned in 2015 by IBM Watson, had originally been developed and spun off by Cleveland Clinic.3 It offered a secure, cloudbased analytics platform leveraging big data for clinical integration, predictive analytics, and business processes.9 Potential uses included analysis of clinical pathways, population health management approaches, outcomes, costs, and reimbursement approaches. Harris described the progression of IT as moving from EPIC for hospital data, to Explorys for system integration, shared knowledge management and affiliated ambulatory services. Payment Clinic charges in 2015 were based on Medicare reimbursement rates and negotiated private payer rates as was the case at most hospitals and health systems. About 43% of Clinic patient volume was insured by Medicare, accounting for 29% of total revenues. Medicaid accounted for 8% of patient volume and 3% of revenues. Managed care and commercial payers together accounted for 43% of patient volume and 61 % of revenues, with the remainder being selfpay or free care. On average, large health plans contracted at rates representing about onethird of posted charges. Some out of state health plans included the Clinic and other leading hospitals in their networks. Patients from outside the region, not covered by a health plan contract with the Clinic either paid posted charges or individually negotiated charges. The Clinic simplified billing for patients by sending a consolidated bill for all hospital and physician services delivered during a hospitalization instead of the widespread practice of multiple bills from different departments and numerous physicians. In 2015, both public and private payers were increasingly using new reimbursement models such as capitation and bundled payment for defined care cycles. As of 2015, the Clinic had 60,000 lives covered in an accountable care organization (ACO) and other contracts with shared savings agreements enabling the Clinic to benefit by achieving cost reductions. Most care, however, was still paid by fee for service. Clinic leaders felt that success in. navigating payment reform required the Clinic to have the capabilities for teams to manage care paths effectively and efficiently across the full care cycle. For some diagnoses, the Clinic had developed bundled payments. The Clinic offered bundled prices directly to employers for hip and knee replacements, treatment of blocked arteries, heart valve repair and vertibroplasty {spine surgery]. Harris explained that when delivery teams created care bundles, costs could be reduced over time, sometimes dramatically. Savings came from fuller or faster recovery, cost reductions identified by the team, and avoiding procedures that did not achieve better outcomes than less invasive approaches. To remain competitive, the Clinic was working to stay ahead of other organizations on this learning curve. Medical Education Cleveland Clinic had long had one of the nation's largest graduate medical education programs, training residents and fellows. In October 2004, the Clinic opened the nation's first new medical school in 25 years, Cleveland Clinic Lerner College of Medicine at Case Western Reserve University. Its program, a year longer than other schools, trained students in both clinical care and research Through its endowment, the Clinic covered the entire cost of tuition for all students beginning in Iuly of 2003. In 2015, the Clinic had 160 medical students, and Dr. Cosgrove offered a position at the Clinic to each graduate. To improve comrnunitybased care and reduce the expected shortage of primary care physicians, the Clinic also had partnered in 2015 with Ohio University's Heritage College of Osteopathic Medicine to develop an innovative curriculum for training more primary care physicians. Heritage had a track record of placing most of its graduates in underserved urban and rural comnumities in Ohio. In 2013, the Clinic and Case Western Reserve University announced construction of an integrated health sciences campus to be built on 11 acres adjacent to the main Cleveland Clinic campus. Colocated in one building, the campus included schools of nursing and dentistry, a physician assistants program and both the Lerner College of Medicine and the Case Western Reserve School of Medicine. Cosgrove explained that the new medical education complex would teach teamwork from the start, rather than train caregivers in separate silos. \"Health care is in the midst of an unprecedented transformation and is changing how we deliver care to patients and howwe getreimhursed for services. . This requires a team of providers with a variety of expertise and experience working together to care for patients and this is why an integrated, medical education program is not just important, but essential." The new programs would use new technologies including the use of holograms and virtual reality technologies instead of cadavers. Also, IBM's Watson computer was being educated in medicine at the Lerner College. ln2015, Watson had assimilated the textbooks and was in the process of learning to read and analyze patients' charts and medical records. Avenues for Growth In the past decade, the Clinic had pursued a number of avenues for growth regionally, nationally, and internationally. Dr. Cosgrove wanted to dene growth areas that aligned medical success with financial success. rI'heClinicprovidedl>5% ofthecareinits county and about25% ofthecaneinthebroader northeastern Ohio region. In its region, the main competitor was the University Hospitals Health System (LII-[HS], also an afliate of Case Western Reserve University. The UHHS system served patients at about 90' locations in northeastern Ohio about 2 million physician visits, 4.5 million outpatient procedures and nearly 63,000 inpatient discharges annually. The Clinic also competed with six smaller health systems in the northeastern Ohio area. The Clinic could potentially expand its presence in Ohio and neighboring states. ClevelandCliniclnnovations (CCDwasformedinZDODasaconmlerdalizationarmandhad enabled 70 new companies. CCI was becoming recognized as a global leader in health IT commercialization 1112011 CCI founded the global health care innovation alliance, making its services available to members, including MedStar Health, North Shore Long Island Jewish Hospital, University of Notre Dame, and others. Dr. Cosgrove reflected that Cleveland did not have a biotech or medical device cluster, but was building a cluster in health IT. In 2001, the Clinic had introduced an online second opinion service, MyConsult that addressed lifethreatening or lifealtering diagnoses. The service reviewed specied information sent in electronically, including notes and digital images, and checked the diagnosis and recommended treatment plan. Between 15% and 20% of the diagnoses reviewed were modied. Nationwide, the rate of diagnostic errors had been estimated at twice that high Statelevel licensing rules meant that the Clinic was required to have physicians licensed in every state in which patients resided. The service had been protable since 2004. As of 2015, MyConsult offered second opinions for over 1,000 life threatening or life-altering diagnoses for a xed fee, serving over 745 patients from around the nation Starting in 2014, the Clinic offered virtual visits at kiosks located throughout greater Cleveland. At the kiosks, attended by a medical assistant, patients could consult an advanced practice nurse or doctor. By following instructions on how to use integrated medical devices within the kiosk, clinicians could listen to the heart, look in the ears or eyes, or examine a rash or swollenjoint. In addition, Urgent and Express Care walkin clinics had been added at many of the 18 Family Health Clinics in the region for timely treatment of minor illnesses and injuries. Clinic leadership was looking for innovative ways to improve access to Cleveland Clinic services, and enhance the value of primary and early stage care. In June 2015, a new service, MyCare Online, began offering secure, ten minute video visits from a smartphone, tablet, or computer. People not already Clinic patients could register online and a physician licensed in the patient' s state would conduct the online visit. Some insurance companies were paying for telemedicine consults. For selfpay patients, an urgent care video visit was $49, while specialty care visits had higher, varying prices. Further expansion of teleamedical offerings was under consideration, including the possibility of webbased telemedical support for physicians in remote locations. Outside of Cleveland, the Clinic's Florida hospitals had historically experienced poor financial performance. In 2006, the Naples hospital was sold and the Clinic bought full ownership of the Weston hospital from its partner, Tenet, a forprofit system based in Dallas, Texas. The Weston hospital was thenintegrated into a unied campus with an associated Clinicdeveloped outpatient practice. By 2008, the Weston campus was running at a profit and at capacity. In 2015, Weston had 229 physicians in 30 specialties. Work to better align the Weston campus with the Clinic as a whole was in process, through knowledge sharing, training, and information systems. Physicians in Weston were formally connected to the Clinic's Institutes, and the culture and strategy of Florida service lines were being aligned with those of the main campus. The Clinic was planning a $300 million expansion of Weston's inpatient facility, referral center services (cancer, cardiac, digestive diseases, neurosciences, and transplant) and outpatient units. The overall plan was to develop Cleveland Clinic Florida into a regional referral center for southeast Florida. The Lou Ruvo Center for Brain Health in Las Vegas, Nevada was opened in 2010. It provided state oftheart care for cognitive disorders and for family members of those who suffered from them. The Center, donated by Las Vegas businessman Larry Ruvo in memory of his father, was dedicated solely to patients with degenerative brain diseases and coordinated the Clinic's research on brain disorders. In September 2015, the Clinic was awarded an $11.1 million federal grant to create a Center for Neurodegeneration and Translational Neuroscience at the Center. In 1994 Dr. Cosgrove had led the creation of a cardiac surgery affiliate program in which surgeons at other hospitals could become Cleveland Clinic staff members and participate in the Clinic's patient registry, quality improvement and training programs, annual performance reviews, and other administrative processes. The first affiliate program began when the cardiac surgeon at EMH Regional Medical Center in Elyria, Ohio died, and the hospital approached the Clinic for help. In 2004, the department added its first outofstate affiliate at a hospital not owned by Cleveland Clinic, with Rochester General Hospital in Rochester, New York. Managed by Dr. Cosgrove and executive administrator Linda McHugh, MBA, the number of patients at affiliates grew rapidly and patient outcomes at affiliates improved to approach the Clinic's own levels. As of 2015, the Clinic operated 14 heart and vascular affiliate programs and 2 in kidney transplant. The heart and vascular affiliates program was the most developed, and included 4 hospitals in Ohio and 15 cardiac groups in other states. The afliate and system hospitals accounted for 59% of the total case volume, with the main campus performing the balance. In the early years of the program, afliated cardiac surgeons sometimes became employees of Cleveland Clinic and practiced under Clinic management. By 2015, the compensation model differed by site and not all of the surgeons were Clinic employees. In return for a fixed fee, the Clinic took over a variety of other functions: physician recruitment and management; support staff (surgical assistants, perfusionists)\" recruitment, education, and management, including training at the main campus if needed; Clinic protocols, procedures, practice guidelines, and patient education materials; technology improvement; joint program marketing and brand development; managed care contracting; insurance, and clinical risk reduction; standardization and procurement of equipment and supplies; quality assurance and results measurement; and overall planning and budgeting. The Clinic had dealt with everything from psychiatric problems with staff to too many wound infections and doctors not answering their pages. Dr. Cosgrove explained, "Every place where we have gone, the quality has risen measurably, and volume has risen.\" Affiliate outcomes improved to at or near main campus outcomes, though afliates tended to operate on patients with fewer risk factors. Affiliates were encouraged to refer particularly difcult cases to Cleveland Clinic or another appropriate hospital. The Clinic was also involved in overall cardiac care at afliates, including program monitoring, intensive care unit monitoring, and management of perfusionists. However, it had not taken over management of cardiology practices or other services in the cardiovascular area. New afliate opportunities were emerging, as surgeons and administrators at other hospitals came forward. The Urological and Kidney Institute also had a smaller affiliate program Relationships with the kidney transplant afliates were based on professional relationships and did not involve employing out of state physicians. In 2013, the Clinic became a founding member of the National Orthopedic and Spine Alliance (NOSA), a collaboration of five independent, highly regarded orthopedic practices. NOSA aimed to market orthopedic surgery to employers and health plans at bundled prices with measured standardized outcomes and appropriateness guidelines. International Expansion The Clinic had long attracted patients from around the world (Exhibit 7), which led to numerous discussions about establishing facilities and partnerships in various countries. In Canada, some citizens traveled to the US. to avoid wait times or for sophisticated services such as heart surgery. The Mayo Clinic and Iohns Hopkins received the largest shares of Canadians based on brand recognition Given Cleveland's proximity, the Clinic opened an executive health and wellness service in Toronto in 2006 to attract more Canadians. The new service provided physical examinations, preventive care and referrals to services at the Clinic or to a Canadian provider, with services at the Clinic paid out of pocket. All 50 of the center staff were Canadian doctors, who had limited relationships with Clinic physicians and knowledge of Clinic services and care processes. Dr. Cosgrove explained, "Our mistake was not introducing enough of our culture and people, and now we need to provide them a transfusion\" In 2010 and 2011, numerous programs and twoway visits by physicians were implemented to infuse culture and build relationships. Over time, revenues were increasing, losses at the Toronto site were declining, and referrals to the main campus increased. The Clinic had also recently created afliations with physician groups in London, Istanbul, and Riyadh as referral sources. In the first 21 months, 425 mostly selfpaying patients were referred. In2006, theClinic began designing and planning construction of a newhospitaLinAbu Dhabi, fully financedbythelocal government. Thegoalwas toti'ansplantinAbuDhabithe"cultureandsoul" of the Clinic's patient care by employing people, process and technology true to Cleveland Clinic ways. The leadership team consisted of six Clinic employees including CEO, Chief Medical Ofcer, Chief Finance Ofcer, Chief Human Resources Ofcer, Chief Information Ofcer and Chief Nursing Ofcer. The Clinic would bring doctors to the U.S. for training, paid for by the local government. [112007,theClinictookovermanagementottheSheikKhalifaMedicalCityinAbuDhabLa com 've health system including a 570bed hospital, 14 specialized outpatient clinics, six family medicine clinics, two urgent care centers, two dental clinics, a blood bank and a 125bed psychiatric hospital. Under Clinic's management, operational improvement had reduced waiting times, improved quality, safety and satisfaction ratings, published outcome measures, piloted an employee wellness program, and converted all facilities to healthy eating zones. As the new Abu Dhabi hospital neared completion in 2011, two senior Clinic MDs, Marc Harrison and Tomislav Mhaljevic, took over leadership. Between 2011 and 2015, they worked to build the culture, operationalize the strategy, and recruit the medical staff. There were 9,000 applications for the 180 physician jobs available. Over 25% of those hired had previously worked at or been trained at Cleveland Clinic, and 5% were Emirati. Eighty percent of the physicians were American certied, and 20% were certified in Western Europe. Annual professional reviews would include the Clinic' 5 key performance indicators. Management was documenting the launch in a playbook that could be used in other locations. In 2015, Harrison became the Chief of International Business Development, with Mihaljevic taking over as CEO of the new hospital. The new Abu Dhabi hospital and outpatient clinic opened for patient care in 2015, with 35 specialties and 55 subspecialties organized in ve centers of excellence based on the needs of the population: Heart and Vascular, Digestive Disease, Respiratory Disease, Eye, and Neurological. In 2015, 75% of patients were Emirati, with 25% coming from other countries. Dr. Cosgrove described the project as an opportunity to improve care and health outcomes for patients in Abu Dhabi, as well as an opportunity for the Clinic to gain expertise in replicating its culture and expertise. The Clinic had also been approached by organizations in many other countries about collaboration In October 2015, the Clinic signed a longterm lease on a sixstory building in the center of London, and management was evaluating what kind of health care services to offer there. Opportunities to expandinlndiaand China, aswell asto acquirehospitals, health systems andinsurersinthe US. were being explored. Dr. Cosgrove would need to decide whether, how and when, to expand further. Exhibit 1 Cleveland Clinic Map CLEVELAND CLINIC REGIONAL HOSPITALS, LAKE COUNTY FAMILY HEALTH CENTERS & HEALTH & WELLNESS CENTERS EUCLID HOSPITAL . Lake Erie O WILLOUGHBY HILLS STEPHANIE TUBBS JONES O HEALTH CENTER LAKEWOOD . HILLCREST HOSPITAL HOSPITAL AVON LAKE Cleveland O BEACHWOOD LAKEWOOD O GEAUGA COUNTY O O LUTHERAN Clinic AVON POINTE RICHARD E. JACOBS HOSPITAL . SOUTH POINTE HOSPITAL HEALTH CENTER, AVON FAIRVIEW CHAGRIN FALLS O AMHERST O SHEFFIELD HOSPITAL MARYMOUNT O LORAIN VILLAGE HOSPITAL O CUYAHOGA COUNTY INDEPENDENCE SOLON O ELYRIA O STRONGSVILLE O TWINSBURG LORAIN COUNTY O BRUNSWICK SUMMIT COUNTY PORTAGE COUNTY MEDINA COUNTY O STOW . MEDINA HOSPITAL OMONTROSE . EDWIN SHAW REHABILITATION . AKRON GENERAL MEDICAL CENTER . LODI COMMUNITY HOSPITAL O GREEN ASHLAND COUNTY WAYNE COUNTY CLEVELAND CLINIC REGIONAL HOSPITALS & FAMILY HEALTH CENTERS . REGIONAL HOSPITAL MAIN CAMPUS O WOOSTER FAMILY HEALTH CENTER HEALTH & WELLNESS CENTER Source: Company documents.Exhibit 2 Cleveland Clinic Total Operating Revenue and Margin %, 1999-2014 Total Operating Revenue and Margin % Billions of Revenue Operating Revenue -Operating Margin % Margins (USD) 8 10.0% 8.0% 6 6.0% 5 4.0% 4 2.0% 3 0.0% 2 -2.0% -4.0% 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 Source: Cleveland Clinic "State of the Clinic."Exhibit 3 Timeline of Selected Cleveland Clinic Innovations in Cardiac Care I 1921: Cleveland Clinic ofcially opened its doors on February 26 I 1932 Cleveland Clinic established a Department of Cardiorespiratory Disease, the forerunner of today' s Heart Center I 1967: Cleveland Clinic heart surgeon pioneered coronary bypass surgery, a new method for ensuring adequate blood ow to the hearts of patients with severe coronary artery disease I 1968: Cleveland Clinic's first heart transplant took place. I 1922 Cardiovascular specialists established a cardiovascular information registry, the world's first computerized registry of data on cardiac diagnosis and treatment I 19805: Cardiothoracic surgeon Delos M. Cosgrove, M.D., developed a computerized device that monitored a patient's condition during recovery from heart surgery and automatically administered drugs as needed. The new device reduced postsurgical complications I 1991: Delos M. Cosgrove, M.D., pioneered aortic valvuloplasty, a procedure that allowed surgeons to repair rather than replace certain diseased heart valves. The procedure enabled better blood ow, minimizes clotting and was especially appropriate for older patients I 1993: The National Institutes of Health designated Cleveland Clinic, one of three centers, to continue research toward developing a totally implantable artificial heart. The Heart Center's Department of Thoracic and Cardiovascular Surgery performed 3420 operations, making it the country's largest openheart surgery center. I 1995: The HeartCenterwasnained'nimiberoneinAmerica' forthersttime inU.S. News&WorldReport's annual 'Bast Hospitals' survey. It remained number one for every year through 2036 I 1996: A Heart Center clinical trial testing implantable cardiac defibrillators in highrisk, postheart attack patients with arrhythmias was stopped early. Cardiothoracic surgeon Delos M. Cosgrove, M.D., performed the world's rst minimally invasive heart valve surgery I 2003: Cleveland Clinic Heart Center Transplant Program completed its 1,CIIIth heart transplant. Only two other hospitals across the nation achieved this milestone, according to the United Network for Organ Sharing I 2006: A new device was developed to'block blood ow to the left atrial appendage, the primary source of stroke in patients with atrial fibrillation. The relative sin'Lplicity of the treatment rrLade an attractive alternative to more complex interventions. I 2006: A multicenter national study led at Cleveland Clinic showed that intensive use of statins resulting in a decreased LDL and increased HDL can reverse the buildup of plaque in coronary arteries. I 2008: Clinic scientists discovered that a specific gene (NUP155), when mutated. was linked to atrial brillation; this may provide a new molecular target to patienttailored treatment strategies. I 2009: The world's rst dual heart and liver transplant was performed on a patient being supported by a total articial heart. I 2011: Surgeons and cardiologists performed the rst transcatheter aortic valve replacement {TAVR) in the United States. I 2011: A team discovered a new pathway that linked a common dietary lipid and intestinal microflora to an increased risk of heart disease, developing a test to measure risk. I 2012 Identification of the master gene regulating the development of blood vessels (angiogetmis) and blood cells. I 2013: Use of smartphonebased heartrhythm monitor for patients who've had ablation for atrial brillation. Exhibit 4 List of Institutes in 2015 CLINICAL INSTITUTES SPECIAL EXPERTISE INSTITUTES . Cancer . Anesthesiology . Dermatology and Plastic Surgery . Arts and Medicine . Digestive Disease . Education . Emergency Services . Imaging . Endocrinology and Metabolism . Nursing . Eye . Pathology and Lab Medicine . Head and Neck . Research . Heart and Vascular . Quality and Patient Safety . Medicine . Neurological . OB and Women's Health . Orthopedic and Rheumatologic . Pediatrics and Children's Hospital . Respiratory . Urological and Kidney . Wellness Source: Cleveland Clinic company documents.709-473 -20- Exhibit 5 Cleveland Clinic Heart and Vascular Institute Outcomes 2014, Table of Contents Heart & Vascular Institute what's inside Chairman's Letter Lung and Heart-Lung Transplant Introduction LO Peripheral Vascular Disease 18 Institute Overview Cerebrovascular Disease Quality and Outcomes Measures Thoracic Surgery Surgical Overview Preventive Cardiology and Rehabilitation 8 Ischemic Heart Disease Sports Cardiology Interventional Treatment Cardio-Oncology Surgical Treatment 16 Surgical Quality
Step by Step Solution
There are 3 Steps involved in it
Step: 1
Get Instant Access to Expert-Tailored Solutions
See step-by-step solutions with expert insights and AI powered tools for academic success
Step: 2
Step: 3
Ace Your Homework with AI
Get the answers you need in no time with our AI-driven, step-by-step assistance