

Question
Introduction: A physician office (private practice) approached you in an effort to convert their paperwork process into a health information database. The physician provided a
Introduction:
A physician office (private practice) approached you in an effort to convert their paperwork process into a health information database. The physician provided a copy of the paperwork used in the office to collect patient information. The physician also explained the need to secure patient information and provided a list of the required level of access for each employee. Additional information will be provided upon request.
The physician would like to add to patient records results from labs and imaging. In addition, the physician would like to link with a list of pharmacies in the area and send the patient prescription electronically. As a database expert, you will be developing a patient database and all required tables using relational database approach.
Requirement:
1.Analyze the provided forms below identifying the entities that should be tracked in the system.
2.Identify the fields (attributes) associated with each entity, listing possible candidate keys (determinants).
3.Based on your analysis and the given forms identify all possible functional dependencies (remember that those functional dependencies will not only assist in creating the proper tables but also will assist in understanding relationships between tables).
4.Create a separate entity to secure database with the list of required level access provided by the physician.
Forms and Documentation Provided:
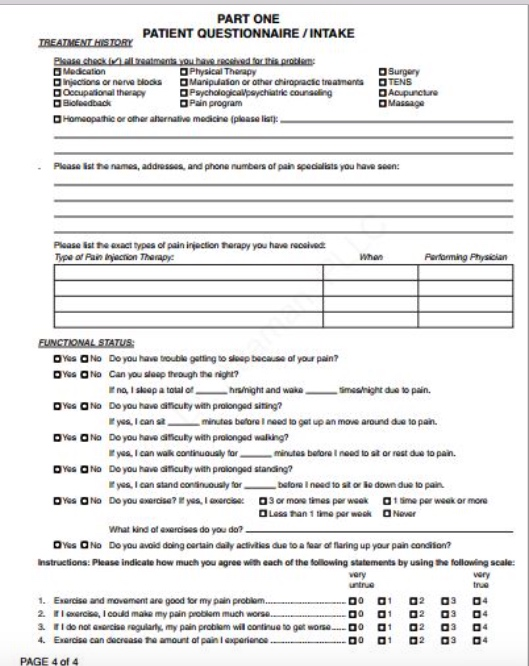
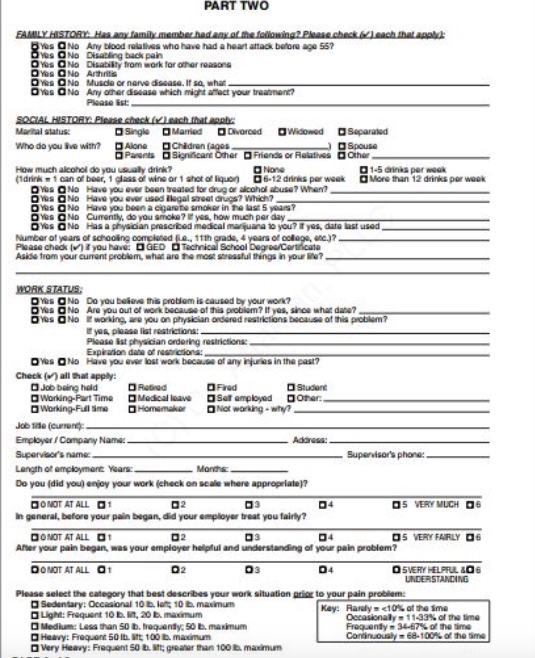
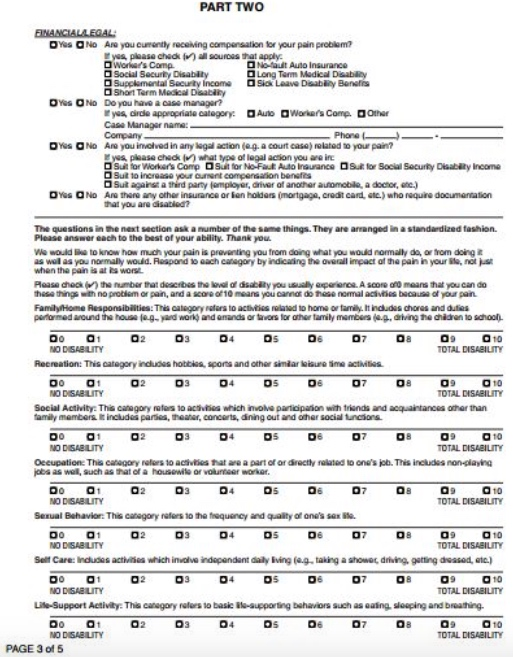
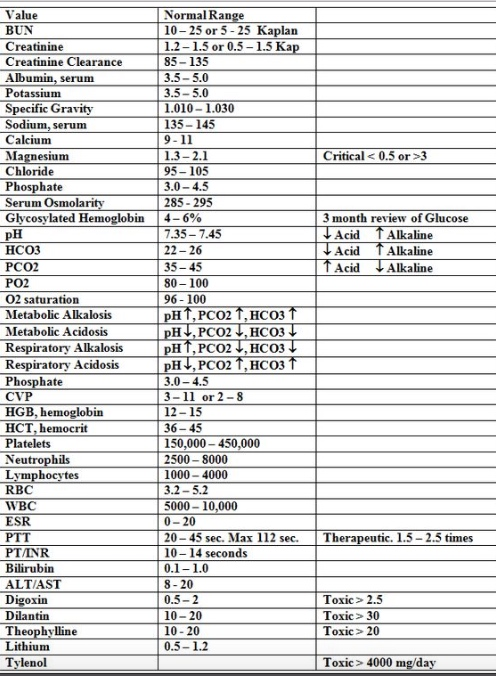
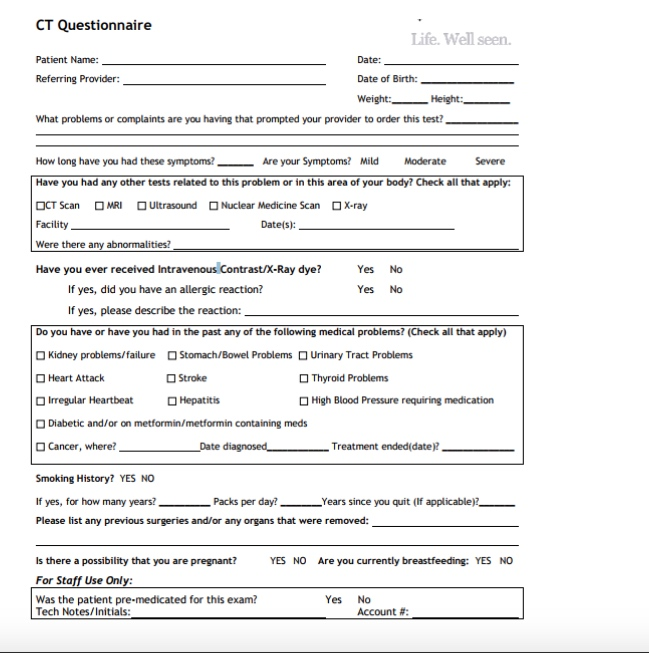
The following are copies of the paper forms used in the office. Use these form to complete the assignment requirements above:
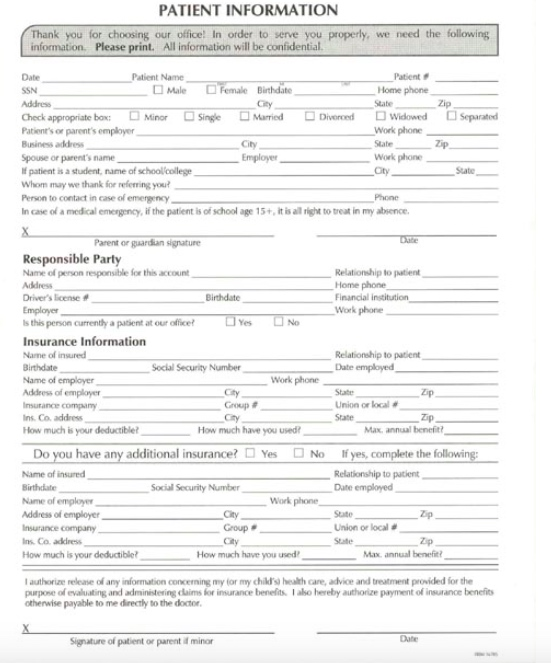
PATIENT INFORMATION k you for choosing our office! In order to serve you properly, we need the following information. Please print. All information will be confidential Patient Home phone Date Patient Name Male Female Birthdate SSN Check appropriate box: Business address Minor Single DDiverod Sparated Dwidowed Work phone State Work phone Mmed Patient's or parent's employer City State- - patient is a student, name of schoollcollege Whom may we thank for referring you Person to contact in case of emergencoy In case of a medical emergency, if the patient is of school age 15+, it is al right to treat in my absence Parent or gaardian signature Responsible Party Name of person responsible for this account Address Driver's leese # Emplayer s this Relationship to patient Home phone Financial institution Work phone Birthdate person currenthy a pasient at our office Insurance Information Name of insured Birthdate Name of employer Relationship to patient Date employed Social Security Number Work phone Address of employe Insurance company ns Co. address How much is your deductiblet Zip Group # Cty Union or local # State How much hav. you used? Max, annual benefit No Do you have any additional insurance? Yes Name of insured Birthdate If yes, complete the following: Relationship to patient Date employed Social Security Number Work phone Name of employe Address of employer Insurance company Ins. Ca. address City Group # City State Union or local # State Zp Max annual benefi How much is your deductible How much have you used I authorize release any rdormation concerning my tor my chikrs health care, advice and treatment provided for the purpose of evalualting and administering claims for insurance benelits1 aso hereby authorize payment of insurance benefit otherwise payable to me direcly to the doctor. Signature of patient or parent if minor PATIENT INFORMATION k you for choosing our office! In order to serve you properly, we need the following information. Please print. All information will be confidential Patient Home phone Date Patient Name Male Female Birthdate SSN Check appropriate box: Business address Minor Single DDiverod Sparated Dwidowed Work phone State Work phone Mmed Patient's or parent's employer City State- - patient is a student, name of schoollcollege Whom may we thank for referring you Person to contact in case of emergencoy In case of a medical emergency, if the patient is of school age 15+, it is al right to treat in my absence Parent or gaardian signature Responsible Party Name of person responsible for this account Address Driver's leese # Emplayer s this Relationship to patient Home phone Financial institution Work phone Birthdate person currenthy a pasient at our office Insurance Information Name of insured Birthdate Name of employer Relationship to patient Date employed Social Security Number Work phone Address of employe Insurance company ns Co. address How much is your deductiblet Zip Group # Cty Union or local # State How much hav. you used? Max, annual benefit No Do you have any additional insurance? Yes Name of insured Birthdate If yes, complete the following: Relationship to patient Date employed Social Security Number Work phone Name of employe Address of employer Insurance company Ins. Ca. address City Group # City State Union or local # State Zp Max annual benefi How much is your deductible How much have you used I authorize release any rdormation concerning my tor my chikrs health care, advice and treatment provided for the purpose of evalualting and administering claims for insurance benelits1 aso hereby authorize payment of insurance benefit otherwise payable to me direcly to the doctor. Signature of patient or parent if minor
Step by Step Solution
There are 3 Steps involved in it
Step: 1

Get Instant Access to Expert-Tailored Solutions
See step-by-step solutions with expert insights and AI powered tools for academic success
Step: 2

Step: 3
Ace Your Homework with AI
Get the answers you need in no time with our AI-driven, step-by-step assistance
Get Started
Database Management System MCQs Multiple Choice Questions And Answers
Authors: Arshad Iqbal
1st Edition
1073328554, 978-1073328550