Q:-1: Why did Johns Hopkins hospital want to develop more resiliency in the nurses? What is the business case? Q:-2:Many of the nurses were initially
Q:-1: Why did Johns Hopkins hospital want to develop more resiliency in the nurses? What is the business case?
Q:-2:Many of the nurses were initially resistant to Applied Improvisation then later found it beneficial. What changed for them?
Q:-3:Where would you benefit from having a greater sense of resilience, and from having those around you feel more resilient?
Thank you so much in advance
Take your time I am here and I will also give you like and comment. Thank You
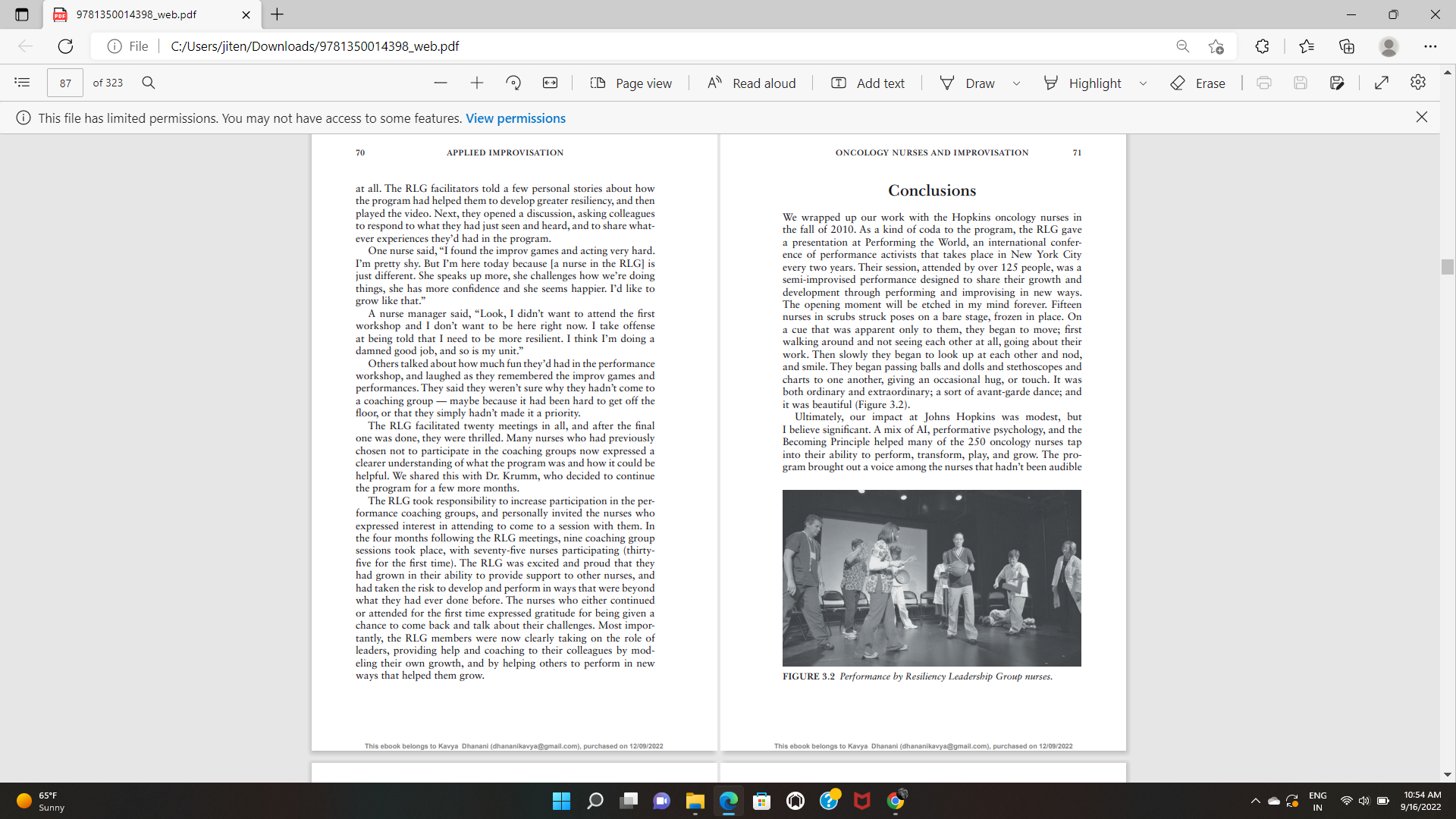
(DE 9781350014398_web.pdf X + X C @ File | C:/Users/jiten/Downloads/9781350014398_web.pdf 71 of 323 Q + Page view A" Read aloud Add text Draw Highlight Erase This file has limited permissions. You may not have access to some features. View permissions X 3 Oncology Nurses Creating a Culture of Resiliency with Improvisation Cathy Salit Cathy Salit is a social entrepreneur, musical comedy improviser, executive coach, and CEO of the training and consulting firm Performance of a Lifetime. She started her career as an innova- tor and upstart at 12, when she dropped out of eighth grade and started an alternative school in an abandoned storefront in New York City. She's a weekly columnist for Inc.com, and her work and thought leadership have been featured in Harvard Business Review, Fast Company, The Wall Street Journal, Forbes, Wired, and Daniel Pink's To Sell Is Human. Cathy is the author of Performance Breakthrough: A Radical Approach to Success at Work (2016). This is a second career for me. I've been a nurse for two years, and I've come to see that I was becoming a protocol, a machine, and the door was closing on my humanity. I didn't know if I could continue to do this work. The arts, This ebook belongs to Kavya Dhanani (dhananikavya@gmail.com), purchased on 12/09/2022 This ebook belongs to Kavya Dhanani (dhananikavya@gmail.com), purchased on 12/09/2022 65.F ENG 10:53 AM sunny IN 9/16/2022(DE 9781350014398_web.pdf X + X C @ File | C:/Users/jiten/Downloads/9781350014398_web.pdf 73 of 323 Q + CD Page view A" Read aloud Add text I Draw Highlight Erase This file has limited permissions. You may not have access to some features. View permissions X 56 APPLIED IMPROVISATION ONCOLOGY NURSES AND IMPROVISATION 57 improvisation and performing are the best way to reconnect requires enormous emotional energy, compassion, and commit- us with our humanity, and I feel like a human being again. ment, and she wanted to give her nursing teams more skills, sup- ONCOLOGY NURSE, THE JOHNS HOPKINS HOSPITAL port, and mastery for managing all the emotional, personal, and social challenges of their jobs. To Dr. Krumm, this meant helping the nurses to develop greater resiliency, which she defined as "a It should come as no surprise to anyone that oncology nursing dynamic process in which healthy skills and abilities enable indi- takes an emotional toll on its practitioners. The stress of dealing viduals to thrive, maintain, and restore personal and professional with gravely ill patients, many of whom don't survive, is easy to well-being."1 imagine. National statistics bear this out, showing that oncology Dr. Krumm went to work, spearheading a Bereavement and nurses experience higher "burnout" rates than any other specialty- Resiliency initiative, funded by a Maryland Health Services Cost including emergency nurses-and lower job satisfaction than nurses Review Commission grant. She started small, offering meditation in general. and yoga classes, and providing a quiet physical space for the nurses Sharon Krumm, PhD, has been the director of Oncology Nursing to take breaks and regroup. It was a good start, but she also wanted at the Sidney Kimmel Comprehensive Cancer Center at the Johns to provide an "intervention" that was interactive and dynamic to Hopkins Hospital since 1988, and for her, the statistics told only help nurses address their emotional needs and give them additional part of the story. The Kimmel Center is one of the country's pre- tools to handle the demands and stress that they faced every day eminent cancer treatment facilities, with a well-earned reputation (and night). for being on the cutting edge of cancer care. As a teaching hos- One day in early 2008, Dr. Krumm attended a presentation at pital and research center, its cancer patients often arrive having a meeting of the Center for Innovation in Quality Patient Care at tried everything else, with cases far more complex than the norm. Hopkins. Karen Davis, at that time the director of nursing for medi- Physicians and nurses there are called upon to make Herculean cine, was reporting on a recent training program for nurse leaders efforts to save their patients, many of whom still die. from both the emergency medicine and general medicine depart- Dr. Krumm was keenly aware of the extraordinary stress her ments. The training had been designed to improve the strained rela- nurses were under, well beyond the fact that burnout was leading to tionships between the two departments, who interfaced regularly high turnover and vacant positions. In 2006, she began conducting during "hand-offs"-transfers of patients from emergency to gen- focus groups and surveys and found that her nurses needed more eral medicine. The program had been a big success, leading not only support in a wide range of areas, including: to greater efficiency and effectiveness of the hand-offs but also to significant improvements in the working relationships between the handling the emotional impact of patients dying; two departments' personnel. While those results were impressive, they weren't all that piqued greater community and collegiality among staff; Dr. Krumm's interest. The program Dr. Davis described was highly an improved mental and physical environment-more unorthodox-it involved play, theatre, and improvisation, and she quiet space, time to eat meals, less clutter, more control of told stories of nurses who had long been frustrated and angry at schedules; and each other now playing and laughing together. And in describing acknowledgment after successfully managing difficult patient all this, Dr. Davis was excited and joyful-which was pretty much situations. unheard of in a data-driven academic setting. I'll have what she's having, Dr. Krumm thought. (She's a big These findings helped Dr. Krumm see that-beyond the structural When Harry Met Sally fan.) What Dr. Davis had been "having" and environmental issues that had to be addressed-something was my company, Performance of a Lifetime (POAL). And that's more personal and developmental was needed. Oncology nursing where our story begins. This ebook belongs to Kavya Dhanani (dhananikavya@gmail.com), purchased on 12/09/2022 This ebook belongs to Kavya Dhanani (dhananikavya@gmail.com), purchased on 12/09/2022 65.F O ENG 10:53 AM sunny IN 9/16/2022(DE 9781350014398_web.pdf X + X C File | C:/Users/jiten/Downloads/9781350014398_web.pdf 75 of 323 Q + 2 0 Page view A Read aloud T Add text Draw Highlight Erase This file has limited permissions. You may not have access to some features. View permissions X 58 APPLIED IMPROVISATION ONCOLOGY NURSES AND IMPROVISATION A Bit of Background language throughout this chapter). We help them grow, learn, and develop by both creating new performances and helping them I'm an improviser, performer, and the CEO of Performance of a to see performance-that they can both be in a scene and see it Lifetime, a consulting and training firm that helps leaders, teams, and unfold; they can write, perform, and direct it simultaneously. They organizations perform and improvise their way to growth, learning, can make creative choices that impact the scene, the characters, and and development. My company's methodological roots stretch back the relationship-all at the same time. As Shakespeare said, "All the to the 1980s, when I began working with people who become my world's a stage," and what makes that world go round is our amaz- lifelong mentors: the developmental psychologist Lois Holzman; ing, creative, and unique ability to perform. the philosopher, psychotherapist, and playwright Fred Newman; and the educator, psychologist, and community organizer Lenora Fulani. Influenced by the work of the early-twentieth-century Soviet A New Kind of Play, for All of Us psychologist Lev Vygotsky, they were making practical-theoretical discoveries in bringing together theatre, improvisation, and thera Dr. Krumm reached out to us shortly after she heard Dr. Davis peutics in efforts for social change, education, and personal growth, speak. Over the spring and summer of 2008, my colleague Maureen a pursuit that has come to be called "performative psychology." Kelly (a brilliant designer, improviser, educator, and social therapist) Founded in the late 1990s, POAL employs an approach we call and I had a series of conversations with her and her assistant direc- The Becoming Principle. Drawing on the discoveries of performa tor, Suzanne Cowperthwaite, to learn as much as we could about tive psychology, the basic idea is this: We humans are all perform the "play" that was being performed daily in the oncology depart- ers, and we collectively create our lives through performing-by ment. It was our version of a needs analysis-we were the observ- simultaneously being who we are and who we're not-that is, who ers (audience) for the everyday occurrences (scenes) taking place in we are becoming. As babies, this comes naturally to us. As children, various units (stages). By the fall of 2008, together with Dr. Krumm we're supported (for the most part) in performing, playing, imagin- and her team, we had roughed out a program design. ing, and improvising; and it's these kinds of activities that account We were excited and nervous about getting under way. Excited, for the rapid learning and development we all experienced when because our observations and conve sations had shown us the enor- we were young. mous stress and pressure that the nurses were under, and we were Unfortunately, for most of us, "growing up" means moving on hopeful that the program could have a meaningful impact on them from that kind of developmental learning. We're told (explicitly and and this pressing healthcare concern. Nervous, because to have implicitly) that it's time to learn the rules, behave properly, know that kind of impact, we had to raise our own game. POAL had what we're doing and how to do it, and figure out (and then be) been working with businesses and nonprofits for about ten years by who we are. Play is relegated to structured contexts (sports, video then, and the principles I articulated above were always the foun- and board games, party games); performing and improvising are dations of our programs. But in improv terms, our work up to this reserved for the professionals. For most adults, "who we're not" is point had been "short-form." We provided a design, customized a stifled. set of exercises to address the client's needs, and created a support- Luckily, our ability to perform, play, and improvise-as ive environment in which they could improvise, play together, and damental catalyst for growing into who we're becoming-never explore new performances. Then, after our day or two together, we goes away. At any time, it can be reignited, and POAL provides all moved on. teams, organizations, and leaders around the world the support This was going to be different. It was "long-form." We were going and direction to do so. We teach them that they are, in fact, nat- to be able to explore and integrate an Applied Improvisational (AI) ural performers, and immerse them in the language of performance approach into the day-to-day activity of nursing at Hopkins over a and improvisation (much as I will be explicitly using performance sustained period. There would be multiple touch points that would This ahook halongs to Kavya Dhanani (dha purchased on 12/09/2022 65.F ENG 10:53 AM sunny IN 9/16/2022(DE 9781350014398_web.pdf X + X C @ File | C:/Users/jiten/Downloads/9781350014398_web.pdf 77 of 323 Q + 2 D Page view A Read aloud T Add text Draw Highlight Erase This file has limited permissions. You may not have access to some features. View permissions X 60 APPLIED IMPROVISATION ONCOLOGY NURSES AND IMPROVISATION inform each other and build over time. And like any long-form But as Applied Improvisers around the world can attest, when performance, it would be unpredictable, with each new moment workshop participants begin to realize that they're not being judged emerging out of what had just been created. It felt risky, challeng or tested or "taught," and that they're really going to play, an invis- ing, and exciting, and had the potential to make a significant dif- ible but palpable burden begins to lift. We're actually allowed to ference for the oncology nurses and to go deeper than anything we laugh and play around here? And we're getting paid to do it? Our (and they) had ever done before. (collective) answer? Yes! Not only are you allowed to play, but you need to play-if you want to grow, learn new things, and create some new tools for resiliency. Part 1: Performance Workshops We kicked off our Performance of Resiliency program in September Upside-Down Introductions 2008. The first "scene" was a mandatory half-day performance workshop, attended by about twenty nurses at a time. Over a One of our (and their) favorite exercises was Upside-Down four-month period, we delivered fifteen of the workshops to dif- Introductions (Workbook 3.1). In pairs, the nurses told each other ferent groups of nurses, offering an intensive immersion into per- about themselves, including why and how they became a nurse. formance and improvisation. Each session was introduced by Then, each introduced their partner to the full group-but did Dr. Krumm or Suzanne Cowperthwaite, who provided an overview so in the first person, playing the role of their partner. Of course, of the Hopkins Bereavement and Resiliency initiative. Then, either the nurses told their partners' stories differently than their part- Maureen or I would give an opening talk in which we set the stage ners would have, and often added insight, color, and nuance that for an unusual four hours. the actual person might not have. This was a surprisingly touch- We introduced the nurses to our approach, and shared that our ing exercise. Hearing someone else share your story "as you" gives focus was twofold-we wanted to both build their resiliency and you (and others) a chance to observe how others see and hear you support them in collectively creating a new "play" for oncology and how they are impacted by you. The upside-down introductions nursing-a resilient, supportive, improvisational ensemble perfor- gave the nurses a direct experience of "being who you are and who mance of their daily work. you're not," and it opened doors for them to express their pride and Then we began performing and improvising together. They passed passion about nursing in a new, improvisational, and collective way. an imaginary ball of energy around a circle, stood in pairs mirror- And through this simple exercise, we saw a caring, open, and col- ing each other's movements, explored different ways of walking laborative ensemble very quickly coming into existence. (from fast to slow to "normal" to slow again), and improvised dif- ferent ways of speaking (using gibberish, using English with pauses, Performing Your Life in One Minute making extended eye contact, and adding silence). We introduced them to the improv principle of Yes, And and other tenets improvis- A centerpiece of each workshop was our signature exercise, the ers adhere to onstage to collaborate, focus, and create connections. One-Minute Performance of a Lifetime, from which we take our While the nurses had been informed that the Performance of name. One at a time, with no advance preparation, we welcomed Resiliency program was going to be "different"-a theatre- and the nurses onto the stage for sixty seconds to "perform their improvisation-based creative and emotional outlet/space and a lives." The subject matter could be anything: from their entire life, chance to open up and talk about their experiences together-they to just the essence of their life, to a single representative moment; were still initially taken aback. Workshops or meetings at Hopkins it could be important or mundane; about being a nurse or not. were typically about policy, process, and new or changed require The only requirement was that it had to be explicitly a perfor- ments. So, at first, they were shy, skeptical, nervous, and confused. mance, not an explanation. We also directed the audience in how This ebook belongs to Kavya Dhanani (dha kavya@gmail.com), purchased on 12/09/2022 This ebook belongs to Kavya Dhanani (dha 65.F ENG 10:53 AM sunny IN 9/16/2022(DE 9781350014398_web.pdf X + X C @ File | C:/Users/jiten/Downloads/9781350014398_web.pdf 79 of 323 Q + CD Page view A" Read aloud Add text I Draw Highlight Erase This file has limited permissions. You may not have access to some features. View permissions X 62 APPLIED IMPROVISATION ONCOLOGY NURSES AND IMPROVISATION 63 to perform the role of audience-as supportive and attentive, usually under tremendous pressure. In one workshop, for example, with enthusiastic applause. a nurse shared her one-minute performance about her father and The nurses' performances were richly varied: some were slices of uncle both being treated on her unit, portraying the stress of trying everyday life, like rushing to leave for work while getting kids ready; to be a nurse, daughter, and niece all at the same time. In the sequel, some were expressions of challenges at the hospital, like a young we created a "nurse chorus" who sang, "How can we be there for nurse's struggle to find a vein for an IV, or a veteran nurse's simple you, now and always?" Afterward, several nurses reflected on how portrayal of caring for a pediatric patient, gently lifting the arm of a she always seemed so strong, "a pillar of strength," and that they toddler and whispering to him tenderly that she needed to give him had no idea she had been struggling. more medicine. Others went further afield-saying goodbye to a Some nurses spoke about their strong commitment-both at grandmother on the eve of emigrating from the Philippines, or a son work and at home-to always being the "helper," and their inabil- trying to communicate with his father who had Alzheimer's. One ity to ask for help from others. They said their "nurse identity" nurse, who had shyly insisted that she wasn't a performer/hated provided a strong sense of self-worth but was also a source of performing/would never perform, told the group she wrote poetry stress. Others talked openly about how, after a patient died, the (which nobody knew) and then performed one of her poems. need to "turn the bed" did not provide time for grieving, or that Following each performance, Maureen and I gave the performer grieving at work was simply not possible: "If I let myself go I may a theatrical direction to improvise and perform beyond what they not be able to pull myself back together. It's better to buck up and had done so far. These short "sequels" were inspired by what we move on." saw, and often included another POAL improviser as a co-performer. While many of the nurses expressed appreciation for the inti- They weren't designed to resolve the conflict of the scene; instead macy of the session, others expressed strong discomfort. When the they revisited, extended, or heightened whatever we wanted to see one-minute performances portrayed personal or emotional events, more of. A few directions we offered were: perform the scene again some nurses said that what their colleagues had shared was "too as a rock-and-roll song with others providing vocal backup; do it much" or was inappropriate in the work environment. These dis- again in your native tongue; try it as a silent modern dance; or play cussions began to show us how high a value many nurses placed on your grandmother this time. the performance of "being strong" and "keeping it together," and By the end of the performances, the group (including Maureen the resiliency-diminishing cost-physical, emotional, spiritual- and me) had traversed the emotional spectrum. Together, we had these choices. Several nurses insisted that compartmentalization and co-created a supportive environment and structure in which the emotional detachment were in fact practical strategies for resilience. nurses performed as they never had before. They worked as a per- From our years of working in healthcare, we knew that this was formance ensemble-exploring, taking risks together, and giving a very common outlook, one that couldn't be ignored. Moreover, one another their honest enthusiasm and appreciation. we were attempting to create a different culture that could include We led the group in reflecting on their experience-an impor- more voices, so we certainly didn't want to shut any down. We tant aspect of the workshop that helped broaden and deepen their would later see some shifts in these attitudes as the nurses observed understanding of what they had just been through. Nurses spoke their colleagues' growth, but at this early stage, we wanted to make about how they had worked together for years, but today learned sure everyone was heard. more about each other than ever before. They expressed their appre- ciation for getting to know nurses from other units, and some spoke about the "old days" when there was more camaraderie across the Post-workshop Follow-Up department. Some talked about how good it was to express their emotions At the end of each of the fifteen sessions, we gave the nurses "resil- and connect differently with people they work with, side-by-side, iency performance homework"-exercises to help them improvise, This ebook belongs to Kavya Dhanani (dhananikavy This ebook belongs to Kavya Dhanani (dhananikavya@gmail.com), purchased o 65.F O ENG 10:53 AM sunny IN 9/16/2022ODE 9781350014398_web.pdf X + X C @ File | C:/Users/jiten/Downloads/9781350014398_web.pdf 81 of 323 Q + D Page view A" Read aloud Add text Draw Highlight Erase This file has limited permissions. You may not have access to some features. View permissions X This ebook belongs to Kavya Dhanani (dhananikavya@gmail.com), purchased on 12/09/2022 This ebook belongs to Kavya Dhanani (dhanani nail.com), purchased on 12/09/2022 64 APPLIED IMPROVISATION ONCOLOGY NURSES AND IMPROVISATION 65 perform, and play in their day-to-day lives, as well as to experiment with some specific new performance choices. Homework included: Walk down the hall very slowly, at least three times a week. When a problem comes up, write a poem about it instead of trying to solve it. . Invite a colleague you don't know to have coffee together. When something goes badly with a coworker, a loved one, or a friend, say, "Let's play that scene over again," and then perform it in a different way. Dr. Krumm also circulated an evaluation to the participants, and on the standard questions about the effectiveness of the instruction, format, and content, the nurses gave 95 percent positive scores. We were especially interested in the comments the nurses pro- vided when asked what they liked most and least about the work. Surprisingly, the same workshop elements-performing, exploring emotions, being pushed out of their comfort zones, and playing games-showed up in equal numbers in both the "most liked" and FIGURE 3.1 Nurses in the Performance of Resiliency program. "least liked" columns. In several instances, nurses listed these activ- ities as what they liked both most and least. I had to smile at that result-anyone who's ever gotten onstage to perform recognizes A typical coaching group session began with warm-up games to that abject dread and profound exhilaration can and do really exist help the nurses to transition from the intensity of work on their unit side by side! to a creative environment (Figure 3.1). One exercise that always had a big impact was I Made a Mistake! (Workbook 3.2), in which participants learn one another's "superhero" names, attempt to flu- Part 2: Performance Coaching Groups idly and correctly identify others' names, and when they make a mistake, they bow, proclaim "I made a mistake!," and receive an Performance coaching groups offered ongoing support in develop- enthusiastic round of applause. ing greater resiliency. They were designed to provide the nurses with When we debriefed the activity, the nurses talked about the a space-a "stage"-for reflecting on their work and lives, and to ways in which they and their units related to mistakes. Some receive (and learn how to give) ongoing support. Participation was described efforts that had been made to provide a space to talk voluntary, and nurses could attend as many sessions as they wanted. about and not hide mistakes. Others spoke about a culture of For two hours, once a month for six months, groups ranging from fear-where there was no way one could admit a mistake, big six to fifteen nurses from different units gathered with Maureen or small. They described "beating themselves up" (and their col- or me. Sessions were loosely structured, allowing us to improvise leagues) in response to life-threatening mistakes but also for the based on the nurses' needs, and-perhaps most importantly- little stuff-being nasty to a colleague, getting frustrated with a create the conditions in which we and the nurses could build the patient, or not doing something perfectly-and the toll this was group into an ensemble. taking on their resiliency. 65.F ENG 10:53 AM sunny IN 9/16/2022PDE 9781350014398_web.pdf X + X C File | C:/Users/jiten/Downloads/9781350014398_web.pdf 83 of 323 Q + 2 CD Page view A Read aloud T Add text Draw Highlight Erase This file has limited permissions. You may not have access to some features. View permissions X 66 APPLIED IMPROVISATION ONCOLOGY NURSES AND IMPROVISATION 67 Improvisational and Emergent it became clear that neither unit knew what the other one did, or Conversations had even been on the other half's floor. They lamented that they felt isolated and didn't have a feel for the bigger picture of oncol- Following the warm-up games, we asked the nurses what they ogy nursing. So, I made what seemed to be the obvious directorial wanted to talk about, get help with, or simply share-the topics were choice (though they initially thought I was nuts). I suggested we do entirely up to them. We explained that we would create the conver- some "research" by taking a tour of their units, a field trip in which sation together, and do exercises or improvise scenes as the need or they'd perform as tour guides for each other in their departments. opportunity arose. At first, most nurses were surprised by how open- I assigned characters and roles to each of the nurses. The newest ended this was. They had expected the performance coaching to be nurses on their unit led the tour, with the direction to speak up with more like a class, and found the loose structure very challenging. confidence and authority. I gave others the role of "the friendly one," We meant it to be. We were asking nurses to be both who they whose objective was to say hello to as many patients and coworkers were and who they weren't. Who they were was professional as possible along our way; and the "curiosity captain," whose role caregivers-highly skilled and empathetic. Who they weren't (yet) was to ask questions and help the group learn more as they toured. was people who felt comfortable not knowing what to do and ask- On one stop of the tour, the thirty-year veteran nurse who handled ing for help. Performing and improvising both the form and the all phone inquiries from chemotherapy outpatients showed us the content of the coaching group sessions would develop their skill closet-like office where she managed what she calls "central com- and comfort with listening, being open, building their relationships, mand." The nurses had no idea how many patients called every day creating trust, and asking for, giving, and accepting help. In this or that one person handled all the calls. For the veteran nurse, this way, it would be part of their becoming more resilient. It was an was the first time her colleagues had ever acknowledged, let alone improv workout for us as facilitators as well! We had to vigorously expressed appreciation for, her work. When the tour was done, the practice what we were preaching: Yes, And everything the nurses session ended with the nurses spontaneously giving each other a said and did; relate to their (and our) mistakes as gifts; and be will standing ovation, hugs, and thanks for their hard work. ing to "go into the cave" of subject matter that was often unex- pected, uncomfortable, or emotionally demanding. Now What? With the freedom (and responsibility) to co-create the coach- ing groups, nurses began to bring many different issues and chal- In March of 2009, the official program was nearing its end, and we lenges they wanted help with, and Maureen and I functioned both could clearly see how the process had impacted the nurses' resil- as coaches and improvisational/theatrical directors. We asked the iency, development, and growth, both individually and as a com- nurses to talk about their experiences when they did the "perfor- munity. A core group of nurses had attended the coaching sessions mance homework" we had assigned in their initial workshop. Some regularly, eagerly bringing in challenges and new performances they had tried new performances and made valuable discoveries, others wanted to work on. They were now using the language of perfor- had tried and "failed," still others had lost their nerve. Whatever the mance and improvisation-Yes, And, accepting and building on outcome, these were offers, and we directed the nurses to respond offers, asking for help, "take two" scenes-and developing close like improvisers, to explore and build on (Yes, And) whatever their relationships across units. These nurses told us they felt stronger, colleagues shared, in order to create greater intimacy and support, more empowered, and happier at work and in life. learn more about one another, and not rush to problem-solving. We But at the same time, participation in the coaching groups had worked with the group as we would with a performing ensemble, been relatively low. Only about a third of the nurses who had and treated their conversations as an improvised play-in-the-making. attended a performance workshop came to one or more group ses- In an early group session, nurses from both the outpatient and sions, and only about 15 percent (a core group of about thirty) inpatient units were talking about their week. Within a few minutes, attended all sessions that were offered. This ebook belongs to Kavya Dhanani (dhananikavya@gmail.com), purchased on 12/09/2022 This ebook belongs to Kavya Dhanani (dhananikavya@gmail.com), purchased on 12/09/2022 65.F ENG 10:53 AM sunny IN 9/16/2022PDE 9781350014398_web.pdf X + X C File | C:/Users/jiten/Downloads/9781350014398_web.pdf 85 of 323 Q + CD Page view A" Read aloud Add text Draw Highlight Erase This file has limited permissions. You may not have access to some features. View permissions X 68 APPLIED IMPROVISATION ONCOLOGY NURSES AND IMPROVISATION We met with Dr. Krumm to discuss possible next steps, if any. The nurses also shared several reasons for the low participation Should we continue Performance of Resiliency in some way? If we in coaching groups. For many nurses, they said, it was just too dif- did, what could we do about the low participation? We didn't want ficult to get off the unit to attend group sessions, and they spoke to make it mandatory or pressure people to come-the last thing candidly about the lack of support from some of the managers. "If these nurses needed was more pressure! We realized-in keeping you're looking for more emotional support but you feel judged by with the improvisational nature of the program-that if we wanted your unit and your manager for that, it's really hard," one com- to build on the offers coming from the nurses, we needed to ask mented. They also said there were some who felt that the program them what they wanted to do. We started by inviting our core group was "too weird," that it was for the "touchy-feely types." One nurse of actively participating nurses, along with Dr. Krumm, to a meet- was philosophical: "It seems that we nurses are at a crossroads. ing to talk about the resiliency program. Did they want to con What does it mean to be a nurse? What can we do with our crea- tinue? What were their thoughts on the low participation? Did they tivity, our emotions?" want to do anything about it, or should we wrap it up at this point and support them in continuing, on their own, with the organic relationships that had evolved? Here are some of the responses: Improvisational Grassroots Democracy "Nurses are constantly in problem-solving and helper mode, At the end of the meeting we asked the core group: What do you and we need a place to stop to see and feel what's happening, want to do? And how can we help? They said they wanted the pro- to not 'have to have it all together,' to share our various emo- gram to continue, to see more of their colleagues participate, and tions. Doing a different kind of performance was both very to try to get more managerial support going forward-and they challenging and helpful." wanted us to teach them how to do all of that. They wanted to put a "I feel more aware of the unit's performance, and not just big question on the table for all the nurses to discuss together: Could my little scene. I work to be more aware of how I talk to col- they create a culture together that would enhance resiliency by help ing one another to-in the words of one nurse-"bring their whole leagues, and see things from the other person's perspective, so self to nursing"? And could they handle their disagreements about I'm not as speedy and reactive in tense situations." this in a way that still grew and developed the community? "Each unit has a different culture and it was helpful to hear This core group of nurses dubbed themselves the Resiliency how other units handled things, and really nice to know that Leadership Group (RLG) and decided to host a series of volun- you were not the only unit struggling with a particular thing. tary meetings in which they could share with their colleagues the It helped to build a sense of solidarity, a connection, across all experiences they had had in the program, explore both the develop- of Oncology Nursing." ment and the disagreements the resiliency program had produced, "These performance coaching groups are very important to and invite their colleagues to participate in coaching groups going me. I don't know if I would have made it through my first forward. They helped us to create a video that included interviews year without the support I got here." with nurses who had participated in and benefitted from the pro- gram, as well as with nurses who did not benefit from the program, Stress relief, emotional support, enhanced community, better did not understand it, or were ambivalent about it.2 teamwork-those had been Dr. Krumm's goals from the start, and We worked with the RLG to prepare them to facilitate the series we were touched and gratified to hear those goals were met. The of meetings, which we also co-designed. Showtime arrived, and four nurses also told us that the program was stimulating conversation nurses from the RLG led the first meeting. They welcomed their beyond the coaching groups, across the entire department, about colleagues, some who had only been to one of the early perfor- what it means to be an oncology nurse, the level of openness that mance workshops, others who had also attended one or two coach was acceptable, and the kind of emotional support that was needed. ing groups, and a handful who had not participated in the program This ebook belongs to Kavya Dhanani (dhananikavya@gmail.com), purchased on 12/09/2022 This ebook belongs to Kavya Dhan ). purchased on 12/09/2022 65.F ENG 10:54 AM sunny IN 9/16/2022PDE 9781350014398_web.pdf X + X C File | C:/Users/jiten/Downloads/9781350014398_web.pdf 87 of 323 Q + 2 D Page view A" Read aloud Add text I V Draw Highlight Erase This file has limited permissions. You may not have access to some features. View permissions X 70 APPLIED IMPROVISATION ONCOLOGY NURSES AND IMPROVISATION 71 at all. The RLG facilitators told a few personal stories about how Conclusions the program had helped them to develop greater resiliency, and then played the video. Next, they opened a discussion, asking colleagues We wrapped up our work with the Hopkins oncology nurses in to respond to what they had just seen and heard, and to share what- the fall of 2010. As a kind of coda to the program, the RLG gave ever experiences they'd had in the program. One nurse said, "I found the improv games and acting very hard. a presentation at Performing the World, an international confer- ence of performance activists that takes place in New York City I'm pretty shy. But I'm here today because [a nurse in the RIG] is just different. She speaks up more, she challenges how we're doing every two years. Their session, attended by over 125 people, was a semi-improvised performance designed to share their growth and things, she has more confidence and she seems happier. I'd like to development through performing and improvising in new ways. grow like that." The opening moment will be etched in my mind forever. Fifteen A nurse manager said, "Look, I didn't want to attend the first nurses in scrubs struck poses on a bare stage, frozen in place. On workshop and I don't want to be here right now. I take offense a cue that was apparent only to them, they began to move; first at being told that I need to be more resilient. I think I'm doing a walking around and not seeing each other at all, going about their damned good job, and so is my unit." work. Then slowly they began to look up at each other and nod, Others talked about how much fun they'd had in the performance and smile. They began passing balls and dolls and stethoscopes and workshop, and laughed as they remembered the improv games and charts to one another, giving an occasional hug, or touch. It was performances. They said they weren't sure why they hadn't come to both ordinary and extraordinary; a sort of avant-garde dance; and a coaching group - maybe because it had been hard to get off the floor, or that they simply hadn't made it a priority. it was beautiful (Figure 3.2). Ultimately, our impact at Johns Hopkins was modest, but The RLG facilitated twenty meetings in all, and after the final one was done, they were thrilled. Many nurses who had previously I believe significant. A mix of AI, performative psychology, and the Becoming Principle helped many of the 250 oncology nurses tap chosen not to participate in the coaching groups now expressed a clearer understanding of what the program was and how it could be into their ability to perform, transform, play, and grow. The pro- gram brought out a voice among the nurses that hadn't been audible helpful. We shared this with Dr. Krumm, who decided to continue the program for a few more months. The RLG took responsibility to increase participation in the per- formance coaching groups, and personally invited the nurses who expressed interest in attending to come to a session with them. In the four months following the RIG meetings, nine coaching group sessions took place, with seventy-five nurses participating (thirty- five for the first time). The RLG was excited and proud that they had grown in their ability to provide support to other nurses, and had taken the risk to develop and perform in ways that were beyond what they had ever done before. The nurses who either continued or attended for the first time expressed gratitude for being given a chance to come back and talk about their challenges. Most impor tantly, the RLG members were now clearly taking on the role of leaders, providing help and coaching to their colleagues by mod- eling their own growth, and by helping others to perform in new ways that helped them grow. FIGURE 3.2 Performance by Resiliency Leadership Group nurses. This ebook belongs to Kavya Dhana mail.com), purchased on 12/09/2022 This ebook belongs to Kavya Dhanani (dhan a@gmail.com), purchased on 12/09/2022 65.F ENG 10:54 AM sunny IN 9/16/2022PDE 9781350014398_web.pdf X + X C File | C:/Users/jiten/Downloads/9781350014398_web.pdf 89 of 323 Q + CD Page view A" Read aloud T Add text Draw Highlight Erase This file has limited permissions. You may not have access to some features. View permissions X 72 APPLIED IMPROVISATION or organized. The leadership group-and the 75 other nurses who joined in again at the invitation of their colleagues-broke from their scripts and constrained roles and performed as who they were not yet by creating an intimate, developing community of support and resiliency. And so, many of the original objectives of the program were met: there was now more teamwork, collegiality, and community among staff-nurses have been able to initiate and deepen relation- ships both within their unit and across their departments. They gained improved communication and support skills and developed a shared language for handling the emotional impact of patients dying. There was more consistent acknowledgment and apprecia- tion after successfully managing difficult patient situations. Years later, I still marvel at all of this. The oncology nurses dis- covered that they could change the play they perform every day. It was a creative and improvisational bringing together of art and sci- ence in how they care for each other as they care for their patients. Notes 1 Personal communication, email 2 To view this video, please visit the Performance of a Lifetime website: http:/ performanceofalifetime.com/clients. 65.F ENG 10:54 AM sunny IN 9/16/2022
Step by Step Solution
There are 3 Steps involved in it
Step: 1
Get Instant Access to Expert-Tailored Solutions
See step-by-step solutions with expert insights and AI powered tools for academic success
Step: 2
Step: 3
Ace Your Homework with AI
Get the answers you need in no time with our AI-driven, step-by-step assistance