Article 1
Doering, L., et al.(2007).Utility of observer-rated and self-report instruments for detecting major depression in women after cardiac surgery: A pilot study.
ARTICLE LISTED ON BOTTOM PAGES 1-9, THEY ARE ALL IN ORDER
1) What was the purpose of the study?
2.) Why is this an important clinical issue?
3) The authors begin by stating that "in adults with coronary artery disease (CAD) depression is common and dangerous."How do the authors support this statement using statistics and what do these statistics mean?
4) If depression after CABG surgery were a benign condition, it might not be particularly important to detect. For example, if the presence of depression was only associated with the type of toothpaste you selected the next day, the toothpaste company might want to fund the study but the National Institute of Health probably would not. Therefore, to strengthen the argument that depression in women after CABG surgery is an important issue to address the nurse researchers need to support that the outcomes associated with the presence of depression are significant. How is statistics used to do thi s ?
5) Now the authors go on to use statistics in another way. They already told us there are few measures of depression in women after CABG surgery but there are reports of rates in a "similar population," those with coronary heart disease or heart failure. Do they report a difference in the gender specific prevalence rates of depression in these women?
6) The researchers then present information about the measurement tools they wish to examine in this study. They already have a valid and reliable tool, the structured diagnostic interview, to detect depression. What do we know about this tool from this description?
7) Why not just keep using this tool if we already know it works?
8) What are the advantages and disadvantages of the self-report and observer instruments used to detect depression?
9) What test is the "gold standard" (the one that will be used to establish that depression exists and test if the other measures are able to detect it)?
10) What type of study design was utilized?
A. Qualitative
B. Quantitative
11) What sampling technique was used?
12) What concerns do you have about the sampling technique?
13) What is the sample size?
14) With the small sample size, what type of error would be most concerning and what would be the result?
A. Type one error
B. Type two error
15) The researchers report that the structured diagnostic interview using DISH (the 'gold standard' for the study) has an inter-rater reliability of 93%. What does this mean about the instrument?
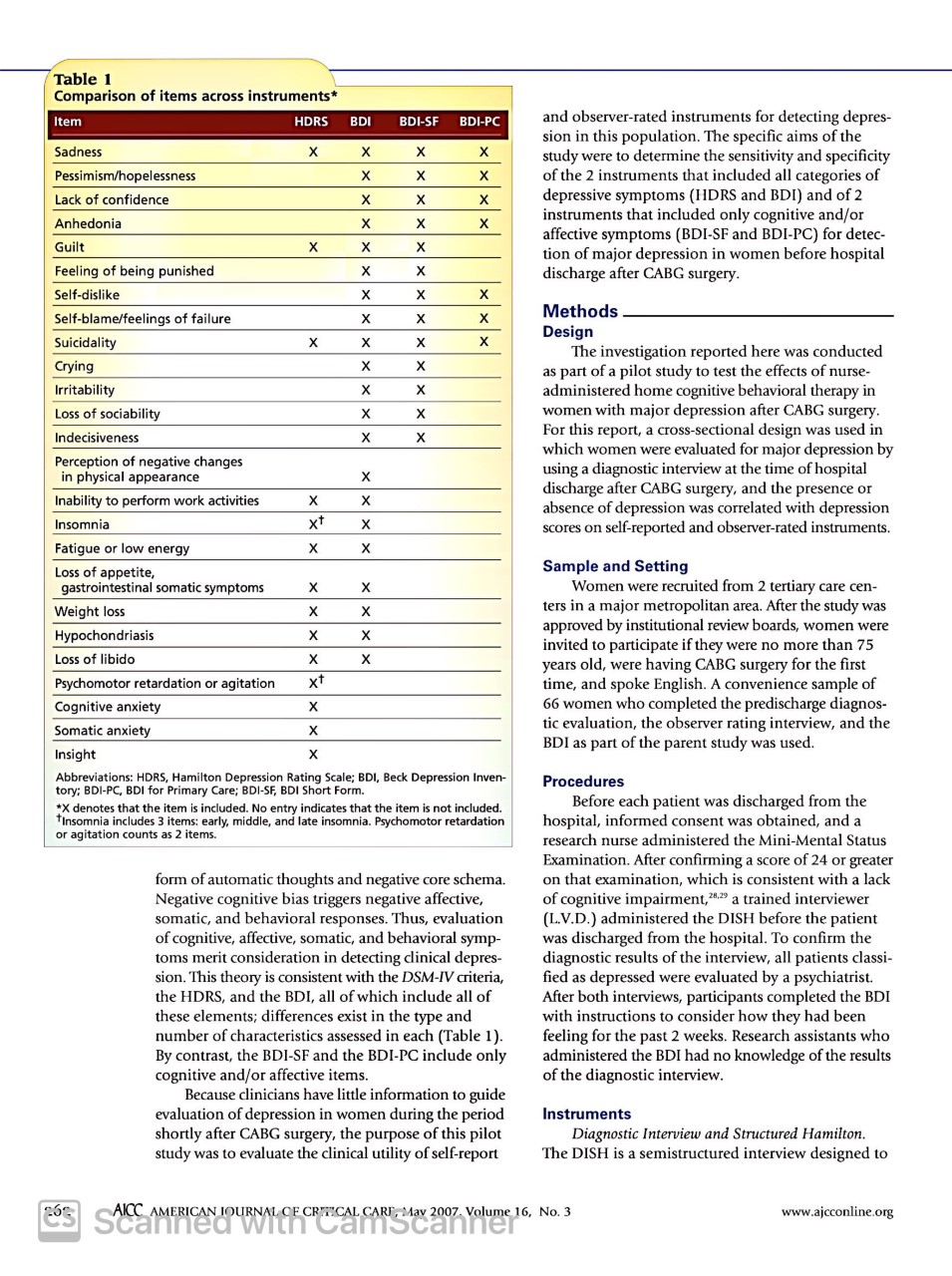
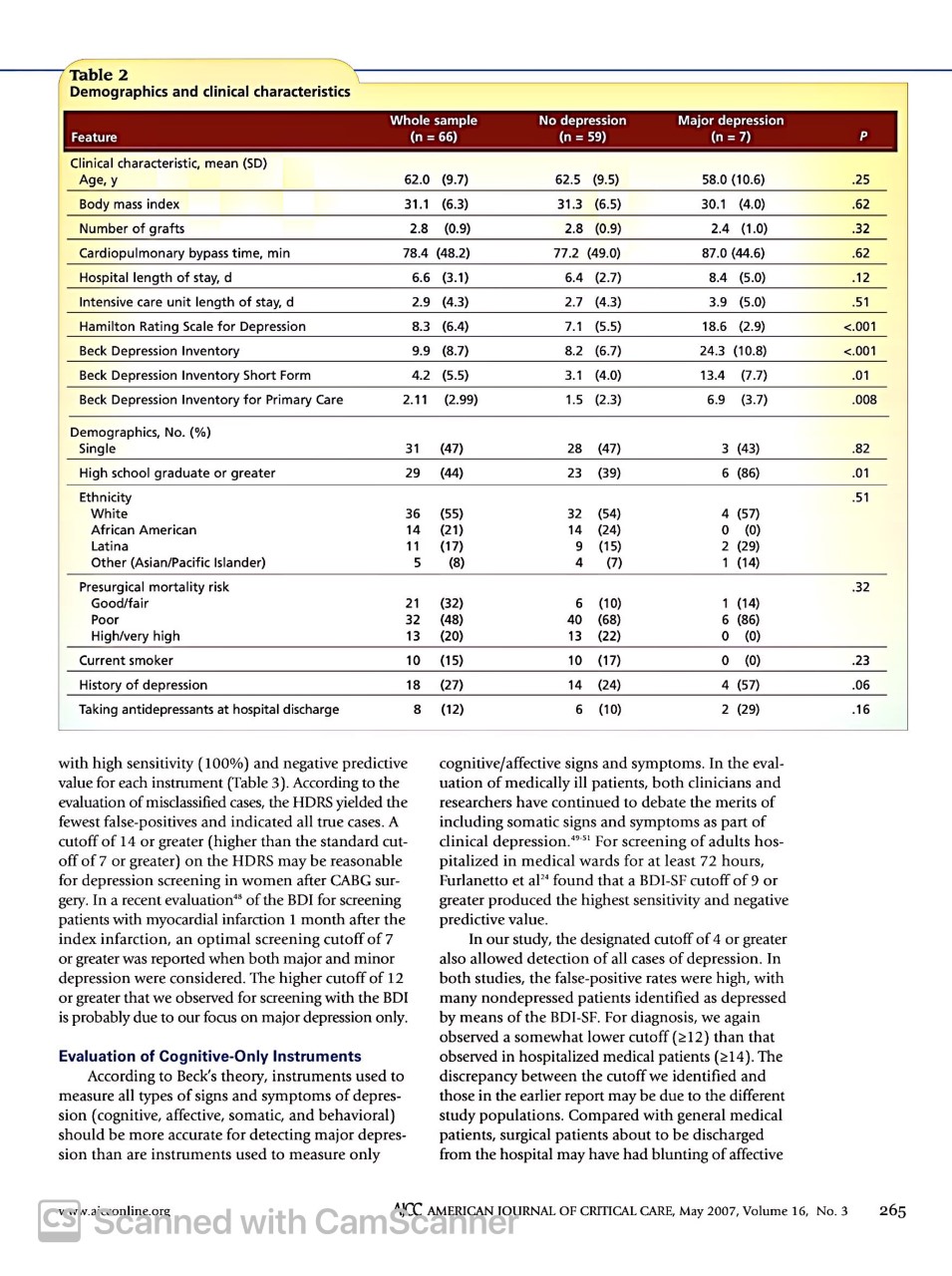
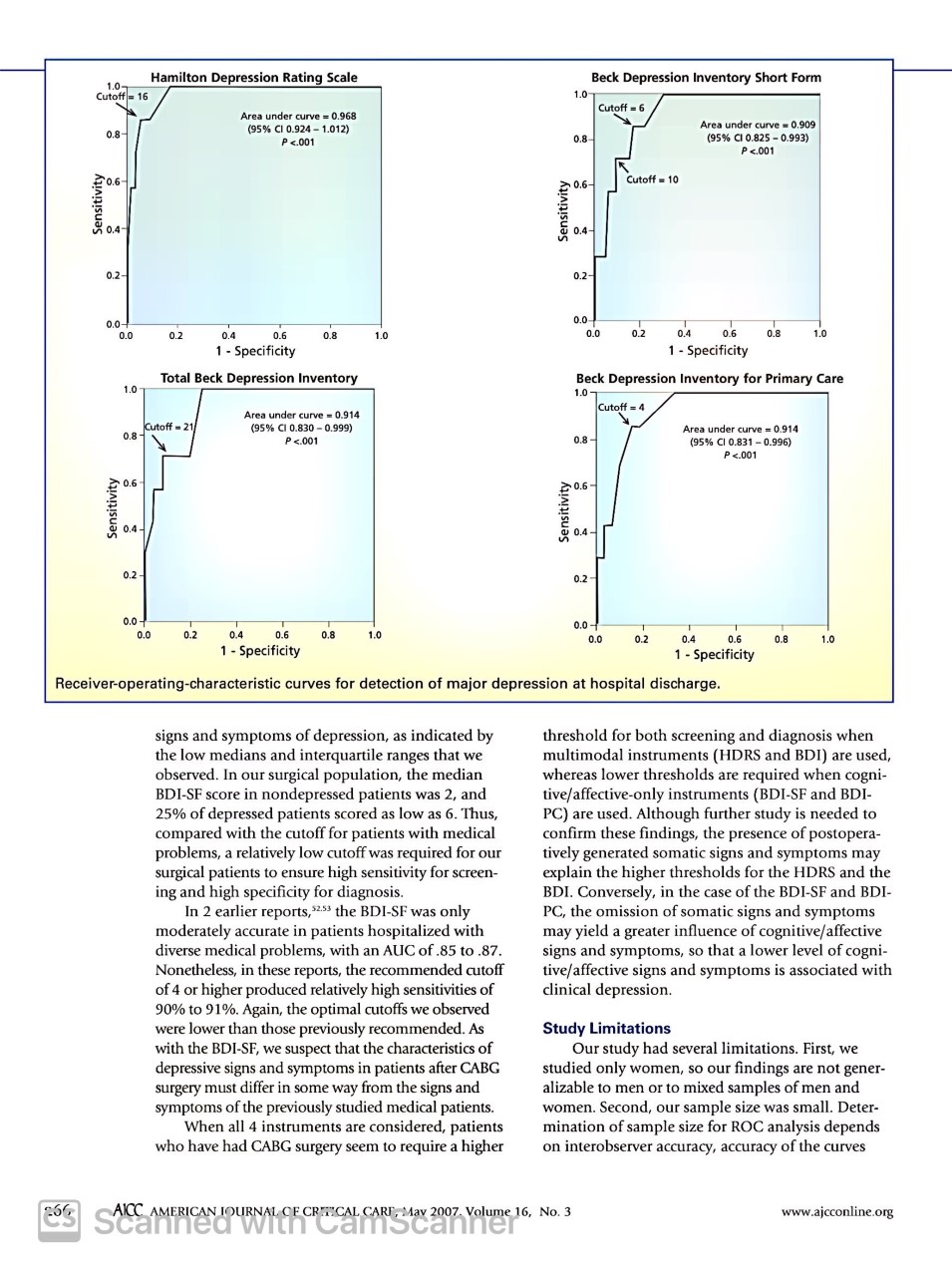
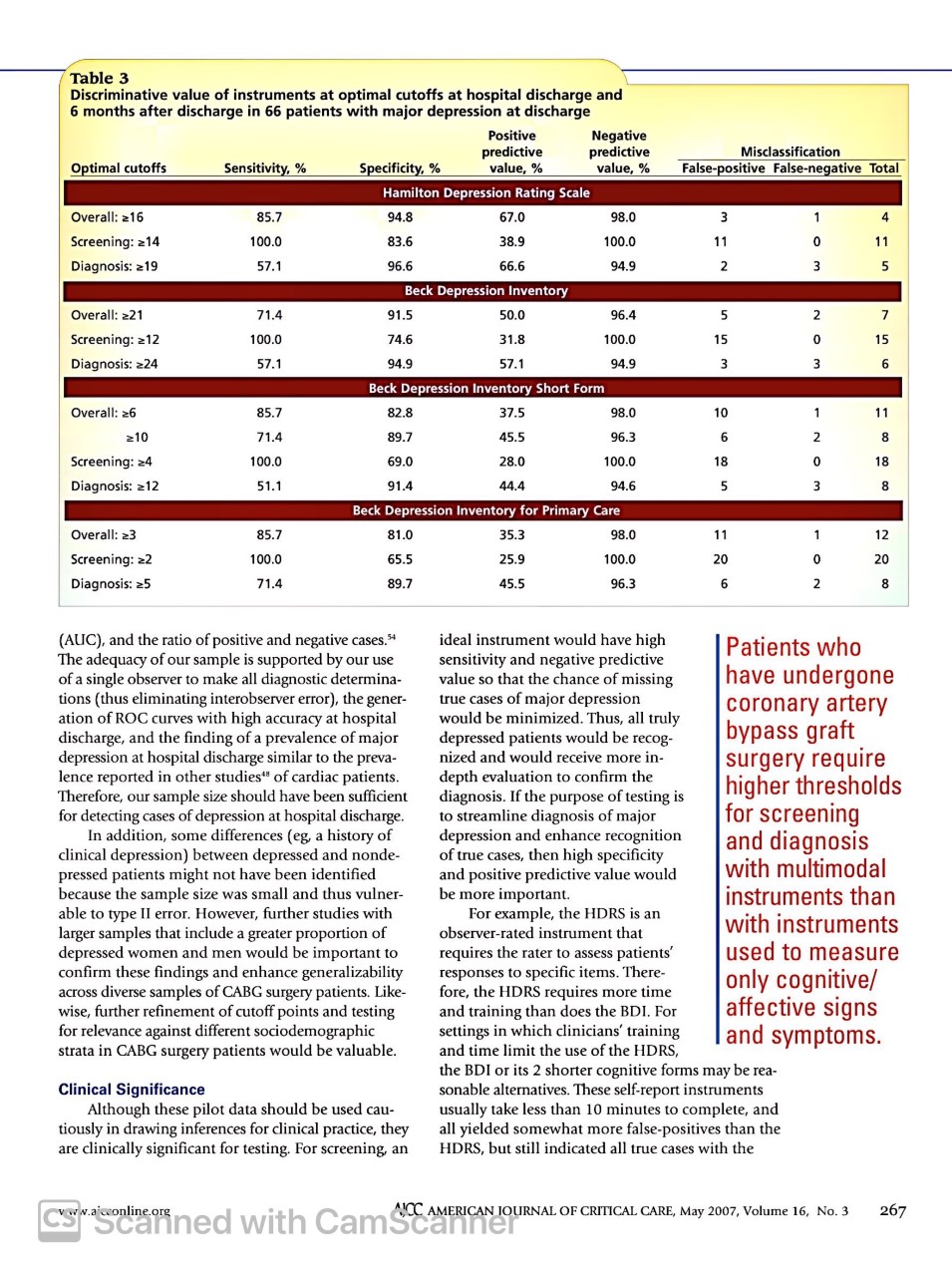
Cardiovascular Issues in Critical Care U TILITY OF OBSERVER- RATED AND SELF-REPORT INSTRUMENTS FOR DETECTING MAJOR DEPRESSION IN WOMEN AFTER CARDIAC SURGERY: A PILOT STUDY By Lynn V. Doering, RN, DNSc, Rebecca Cross, RN, MSN, FNP, Marise C. Magsarili, RN, MN, Loretta Y. Howitt, MD, and Marie J. Cowan, RN, PhD Background Major depression is common after coronary artery bypass graft surgery and is associated with increased mortality and morbidity. Clinicians have few practical options for detecting depression, especially in women, who are at higher risk for depression than men. Objectives To evaluate the clinical utility of common self-report and observer- rated instruments for detection of major depression in women after coronary artery bypass graft surgery. Methods In 66 women being discharged after coronary artery bypass graft surgery, 4 instruments were completed: the Hamilton Depression Rating Scale, Beck Depression Inventory, Beck Depression Inventory Short Form, and Beck Depression Inventory for Primary Care. For each instrument, receiver-operating- characteristic curves were analyzed, and positive and negative predictive val- ues were calculated for cutoff points determined from the curves Results At hospital discharge, all 4 instruments yielded highly accurate curves. Compared with cutoffs suggested for patients without medical illness and hos pitalized nonsurgical patients, identified cutoffs for screening were higher when all types of depressive symptoms (cognitive, affective, behavioral, somatic) were measured with the Hamilton Depression Rating Scale and the Beck Depression Inventory but lower when only cognitive and/or affective symptoms were measured with the 2 subscales of the Beck Depression Inventory. Conclusions The Hamilton Depression Rating Scale and both subscales of the Beck Depression Inventory may be useful for detecting major depression in women shortly after coronary artery bypass graft surgery. Further study is war- ranted to confirm cutoffs in these patients. (American Journal of Critical Care. 2007;16:260-269) AJCC AMERICAN JOURNAL OF CRITICAL CARE, way 2007. Volume 16, No. 3 www.ajcconline.org scanned with camscannern adults with coronary artery disease, depression is common and dangerous." Adults undergoing coronary artery bypass graft (CABG) surgery are particularly susceptible; signs and symptoms of depression are extremely common both before and after surgery. 3. Prevalence reports range from 32% to 65% for signs and symptoms within 1 week before surgery and from 20% to 46% for signs and symptoms measured up to 6 months after surgery." Clinical depression after CABG surgery has rarely been described; 17% to 20% of patients have postoperative major depression, and an additional 27% of patients have minor depression."In contrast, the 12-month prevalence of major depression in community samples of adults is 5.5% to 10.8%.",10 With approximately 306000 patients undergoing CABG surgery annually in the United States, " approximately 61000 of them are likely to experience major depression. Depressed patients, compared with nondepressed patients, have a higher rate of depression-related mortality and morbidity after CABG surgery, more cardiac events and post- operative complications such as hospital readmissions, and higher healthcare costs. 7,12.14 In general, rates of depression in women are depression, especially in women. Structured diagnostic higher than the rates in men, and outcomes in women interviews, such as the Diagnostic Interview and tend to be worse." Although few reports address Structured Hamilton (DISH) or the Structured Clinical depression in women after CABG surgery, rates of Interview for the Diagnostic and Statistical Manual, depression in women with ischemic heart disease Fourth Edition (DSM-IV), are well validated and and women with heart failure follow this general reliable but require extensive training and are time- pattern. Among patients with heart failure, women consuming to administer. 21 22 Alterna- are more likely to be depressed than men, and tively, self-report and observer Depression depressed patients tend to be younger than nonde- instruments have the advantage of pressed patients." being short and easier to use than increases In the Enhancing Recovery in Coronary Heart structured interviews, but most were mortality, cardiac Disease trial, female patients reported higher levels of designed to measure the severity of events, and depression and distress than did male patients; the signs and symptoms of depression greatest differences occurred among younger only rather than clinical depression. postoperative women." In women undergoing CABG surgery, Among self-report instruments, complications depression occurs at rates similar to the rates in the Beck Depression Inventory (BDI) women with heart failure and the rates in other clin- is considered the reference standard." after coronary ical populations, such as women with diabetes. 1519 Although it was originally developed artery bypass Compared with men, women may be particularly for use in psychiatric patients, the BDI susceptible to depression after CABG surgery because has been widely used in both healthy surgery. women tend to become depressed after a triggering and medically ill populations. Recently, new subscales event, such as surgery." of the BDI for use with medically ill patients have Despite the prevalence of depression after CABG been developed, including a 13-item version of all surgery and its association with mortality and morbid- cognitive/affective items in the BDI, called the BDI ity, clinicians have few practical options for detecting Short Form (BDI-SF)," and a 7-item version of selected cognitive/affective items, called the BDI for Primary Care (BDI-PC)." Among observer-rated instruments, About the Authors the Hamilton Depression Rating Scale (HDRS) is Lynn V. Doering is an associate professor, Rebecca Cross the most widely accepted." Like the BDI, the HDRS is a doctoral candidate, and Marie J. Cowan is a profes- sor and dean in the University of California-Los Angeles has been used widely in medically ill populations. School of Nursing. Marise C. Magsarili is a nurse practi- Beck's cognitive model of depression offers an tioner and Loretta Y. Howitt is a physician with Kaiser appropriate theoretical framework for evaluating Permanente Medical Center in Los Angeles, Calif. these instruments." Beck postulates that depressed Corresponding author: Lynn Doering, RN, DNSc, FAAN, UCLA individuals have a negative bias in their view of School of Nursing, 700 Tiverton Ave, Factor 4-266, Los themselves, their world, and their future. This nega- Angeles, CA 90095-6918 (e-mail: Idoering@sonnet.ucla.edu). tive bias is evident in their cognitive function, in the Cygov.afcconline.org Scanned with CamScanner AICC AMERICAN JOURNAL OF CRITICAL CARE, May 2007, Volume 16, No. 3 261Table 1 Comparison of items across instruments* Item HDRS BDI BDI-SF BDI-PC and observer-rated instruments for detecting depres- sion in this population. The specific aims of the Sadness X X X X study were to determine the sensitivity and specificity Pessimism/hopelessness X X X of the 2 instruments that included all categories of Lack of confidence X X X depressive symptoms (HDRS and BDI) and of 2 Anhedonia X X X nstruments that included only cognitive and/or Guilt X X X affective symptoms (BDI-SF and BDI-PC) for detec- ion of major depression in women before hospital Feeling of being punished X X discharge after CABG surgery. Self-dislike X X X Self-blame/feelings of failure X X X Methods Suicidality X X X X Design The investigation reported here was conducted Crying X X as part of a pilot study to test the effects of nurse- Irritability X X administered home cognitive behavioral therapy in Loss of sociability X X women with major depression after CABG surgery. Indecisiveness X X For this report, a cross-sectional design was used in which women were evaluated for major depression by Perception of negative changes in physical appearance X using a diagnostic interview at the time of hospital X discharge after CABG surgery, and the presence or Inability to perform work activities X absence of depression was correlated with depression Insomnia xt X scores on self-reported and observer-rated instruments. Fatigue or low energy X X Loss of appetite, Sample and Setting gastrointestinal somatic symptoms X X Women were recruited from 2 tertiary care cen- Weight loss X X ters in a major metropolitan area. After the study was Hypochondriasis X X approved by institutional review boards, women were Loss of libido X X invited to participate if they were no more than 75 years old, were having CABG surgery for the first Psychomotor retardation or agitation xt time, and spoke English. A convenience sample of Cognitive anxiety X 56 women who completed the predischarge diagnos- Somatic anxiety X ic evaluation, the observer rating interview, and the BDI as part of the parent study was used. Insight X Abbreviations: HDRS, Hamilton Depression Rating Scale; BDI, Beck Depression Inven- tory; BDI-PC, BDI for Primary Care; BDI-SF, BDI Short Form. Procedures *X denotes that the item is included. No entry indicates that the item is not included. Before each patient was discharged from the TInsomnia includes 3 items: early, middle, and late insomnia. Psychomotor retardation hospital, informed consent was obtained, and a or agitation counts as 2 items. research nurse administered the Mini-Mental Status Examination. After confirming a score of 24 or greater form of automatic thoughts and negative core schema. on that examination, which is consistent with a lack Negative cognitive bias triggers negative affective, of cognitive impairment,"a trained interviewer somatic, and behavioral responses. Thus, evaluation (L.V.D.) administered the DISH before the patient of cognitive, affective, somatic, and behavioral symp- was discharged from the hospital. To confirm the toms merit consideration in detecting clinical depres diagnostic results of the interview, all patients classi- sion. This theory is consistent with the DSM-IV criteria, fied as depressed were evaluated by a psychiatrist. the HDRS, and the BDI, all of which include all of After both interviews, participants completed the BDI these elements; differences exist in the type and with instructions to consider how they had been number of characteristics assessed in each (Table 1). feeling for the past 2 weeks. Research assistants who By contrast, the BDI-SF and the BDI-PC include only administered the BDI had no knowledge of the results cognitive and/or affective items. of the diagnostic interview. Because clinicians have little information to guide evaluation of depression in women during the period Instruments shortly after CABG surgery, the purpose of this pilot Diagnostic Interview and Structured Hamilton. study was to evaluate the clinical utility of self-report The DISH is a semistructured interview designed to AICC AMERICAN JOURNAL OF CRITICAL CART, May 2007. Volume 16, No. 3 www.ajcconline.org Scanned with camscannerdiagnose depression in medically ill patients." In and negative predictive value (100%) in patients validation studies, the DISH and Structured Clinical hospitalized in a general medical ward." With a cut- Interview for DSM-IV resulted in 88% agreement off of 8 or greater, the BDI-SF had adequate sensitive (K =.86)." Interrater reliability has been established, ity (79%) and negative predictive value (96%) with with 93% agreement between diagnosis by trained diagnostic interviews in a sample of terminally ill interviewers and clinicians and with diagnostic cancer patients receiving palliative care and was well agreement across symptom clusters (K =.75).21.30 correlated (r=0.96) with the original 21-item scale." Beck Depression Inventory. The BDI is a 21-item self- In the study reported here, tests of internal consis- reported measure of the intensity of signs and symp- tency yielded a Cronbach a coefficient of .89. toms of depression, with items rated 0 to 3 (0 = no Beck Depression Inventory for Primary Care. Like signs or symptoms, 3 = most severe signs and symp- the BDI-SF, the BDI-PC was designed to minimize toms) and totals ranging from 0 to 63 (Table 1). the possibility of yielding spuriously high estimates Suggested guidelines for cutoff scores are less than of depression in patients with medical illnesses by 10 for no or minimal depression, 10 to 18 for mild focusing on cognitive/affective signs and symptoms. to moderate depression, 19 to 28 for moderate to For the BDI-PC, 7 items were selected purposively to severe depression, and 29 and higher for severe correspond to DSM-IV criteria (sadness and anhedo- depression. The BDI is used routinely to monitor nia), to capture important clinical indicators of risk changes in signs and symptoms in cognitive behav- in depressed patients (suicidality), and to reflect ioral therapy. Concurrent validity of the BDI has those items that loaded most saliently (2.35) on the been supported by correlations between the BDI cognitive dimension of the original instrument (pes- and selected concurrent measures of depression and simism, past failure, self-dislike, and lack of confi- by agreement with clinical psychiatric evaluations of dence)." As with the BDI and BDI-SF, the items are depression." Meta-analyses of internal consistency scored from 0 to 3 to reflect intensity of the sign or have yielded Cronbach a coefficients of .86 for psy- symptom, but the BDI-PC includes only 7 items. chiatric patients and .81 for nonpsychiatric patients." Totals range from 0 to 21. A cutoff Among CABG patients, internal consistency of of 4 and higher yields strong sensi- the BDI is high, with Cronbach a coefficients of .82." Women with tivity (82%-83%) and specificity Widely used to assess the severity of depression in (82%-95%) rates for detection of heart failure are psychiatric patients, the BDI also has been validated major depression in medical inpa- more depressed in older adults" and across a variety of medical pop- ients and outpatients.254 In the study ulations, including patients with diabetes" or chronic reported here, tests of internal con- than men, and pain" and patients undergoing hemodialysis." The sistency yielded a Cronbach a coef- depressed BDI has demonstrated utility for differentiating among ficient of .87. medical, nonmedical, and healthy groups" and is a Hamilton Depression Rating Scale. patients are sensitive indicator of cardiac mortality." It has shown The 17-item version of the HDRS is younger than discriminative validity in distinguishing higher from administered via a structured inter- nondepressed lower sympathetic nervous activation in women view in which subjects are asked to tested for severity of depressive symptoms." In the respond to questions about the signs patients. study reported here, tests of internal consistency and symptoms they had during a yielded a Cronbach a coefficient of .92. specific (2-week) period (Table 1). Responses are Beck Depression Inventory Short Form. The BDI-SF rated by the interviewer, with 8 affective/cognitive includes all 13 cognitive/affective items in the BDI items rated on a 5-point scale (0=no signs or symp- (Table 1). The BDI-SF was developed in response to toms, 4 = most severe signs and symptoms) and 9 concerns that in medically ill populations the use of somatic items rated on a 3-point scale (0 = no signs somatic items to evaluate depressive symptoms might or symptoms, 2= most severe signs and symptoms) lead to spuriously high scores and overreporting of Scores range from 0 to 52. Scores of 24 or higher are depression." As with the BDI, items are scored from 0 generally agreed to indicate severe depression, whereas (no signs or symptoms) to 3 ( most severe signs and scores of 18 to 23 represent the moderate range, 7 to symptoms); total scores range from 0 to 39. The use 17 signify mild depression, and scores less than 7 of only the cognitive/affective items was suggested to indicate no depression." The HDRS is sensitive to assess depression in medically ill patients, with the change over time and treatment and agrees well use of scores of 10 or greater as a cutoff for moderate with overall clinical ratings of severity." It has well- to severe depressive syndromes." With this cutoff, documented validity, with a Cronbach a of .81 recently the BDI-SF has demonstrated high sensitivity (100%) reported"; recent studies also support interrater Cygow.ajcconline.org Scanned with CamScanner ACC AMERICAN JOURNAL OF CRITICAL CARE, May 2007, Volume 16, No. 3 263reliability, with intraclass correlations of 0.96 to at hospital discharge, the administration of aspirin, 0.97.45." For this study, administration time for the B-blockers, statins, and hormone replacement ther- HDRS was approximately 30 minutes. apy did not differ significantly between groups. For the whole sample, median scores for the Analysis HDRS, BDI, BDI-SF, and BDI-PC were 8, 8, 2, and 1, Measures of central tendency and dispersion were respectively. Interquartile ranges (25%-75%) for the used to describe the sample. For comparing depressed instruments were 3 to 13.25, 3 to 13, 0 to 5.5, and 0 with nondepressed patients, a t test was used for con- to 3, respectively. For the HDRS, 55.4% of patients tinuous variables and a x2 test for categorical vari- scored at or above the usually accepted cutoff for ables. For each of the instruments and subscales nonmedically ill patients of 7. For the BDI, 43.9% (HDRS, BDI, BDI-SF, and BDI-PC), receiver-operat- scored 10 or higher, the recommended cutoff for ing-characteristic (ROC) curves were analyzed to gen- depressive symptoms in nonmedically ill patients. erate plots of sensitivity versus 1 minus specificity for For the BDI-SF and the BDI-PC, 20% and 23.1% detecting major depression for every possible cutoff scored above the cutoffs of 8/9 and 4, respectively, point and to generate graphs of the area under the recommended for medically ill patients.2" With all curve (AUC). The AUC is equivalent to the probabil- 4 instruments, scores of depressed and nondepressed ity that a randomly selected individual from the pos- patients differed significantly (Table 2). itive reference sample has a greater test value than a The Figure presents the ROC curve analyses for randomly selected individual from the negative ref- detection of major depression at hospital discharge. erence sample; an appropriate sample estimate is All 4 instruments yielded strong ROC curves, with made by using the nonparametric Mann-Whitney U AUCs exceeding .900 considered highly accurate.* test." Curves are ranked against noninformative Cutoff points derived from each curve were exam- curves as less accurate (0.5
2) but indicated all depression), we examined each curve han previously reported (BDI-SF2 8, BDI-PC24). true cases. for cutoff points that would maximize Similarly, diagnostic cutoffs for these instruments sensitivity and negative predictive value (BDI-SF 2 12, BDI-PC25) were lower than those (for screening) and specificity and previously reported (BDI-SF 2 13, BDI-PC2 6). positive predictive value (for diagnosis). Discussion Results. To our knowledge, this is the first study in which Characteristics of the sample as a whole and by the BDI and its shorter cognitive-based forms, along depression status at hospital discharge are presented with the HDRS, were evaluated concurrently in in Table 2. At hospital discharge, 7 women (11%) medically ill patients. At the time of patients' discharge met the diagnostic criteria for major depression; of from the hospital after CABG surgery, all 4 instru- these, 4 had a history of depression (P=.06). Com- ments yielded ROC curves consistent with highly pared with women without depression, depressed accurate tests, with AUCs exceeding .900. These data women were less educated (P=.01). Preoperative risk provide important albeit initial support for the util- did not differ significantly between groups. During ity of all 4 instruments as tests for major depression hospitalization, the rates of complications, include at the time of hospital discharge after CABG surgery. ing incidence of perioperative myocardial infarction Although these data are encouraging, further analysis and acute renal failure, were similar in depressed and in larger studies is needed to confirm these findings. nondepressed women. Women with major depression at discharge had experienced longer periods of postop- Evaluation of HDRS and BDI erative intubation than had women without depression For screening, on the basis of the ROC curves at (28.6% vs 5.2%, P=.03). Regarding medical treatment hospital discharge, we were able to identify cutoffs AICC AMERICAN JOURNAL OF CRITICAL CART, May 2007. Volume 16, No. 3 www.ajcconline.org Scanned with camscanner't '_'\\.\\ Whole sample i-Jct depression Major tie pression {n = as) {n = 59) (n = in Clinical characteristic. mean (50} Age, y 62.0 {9.3"} 62.5 [9.5) 58.0 (10.6) .25 Body mass index 31.1 {6.31 31.3 (6.5) 30.1 {4.01 .62 Number of grafts 2.8 (0.9} 2.3 (0.9) 2.4 (1.0) .32 Cardiopulmonary bypass time. min 3'81 (43.2] 1'12 {49.01 310 (44.6) .62 Hospital length of stay, cl 6.6 {3.1) 6.4 {2.7) 3.4 (5.0} .12 Intensive care unit length of stay. d 2.9 {4.3) 2.? {4.3) 3.9 (5.0} .51 Hamilton Rating Scale for Depression 6.3 {6.4) 7.1 {5.5) 18.6 {2.91 c.0111 Beck Depression Inventory 9.9 (8.7) 8.2 {6.7) 211.3 (10.0) <.0 beck depression inventory short form .01 for primary care .000 demographics no. wu single .32 high school graduate or greater ethnicity .51 white african american u latina other islander t7 presurgicai mortality risk goodair e poor higlvvery current smoker .23 history of .06 taking antidepressants at hospital disdtarge .16 with sensitivity and negative predictive cognitive affective signs symptoms. in the eval- value each instrument according to nation medically ill patients both clinicians evaluation misdassied cases hdrs yielded researchers have continued debate merits fewest false-positives indicated all true cases. a including somatic symptoms as part cutoff than standard ctll- clinical depression.ml screening adults hos- o i on maybe reasonable pitalized medical wards least hours. women after cabg sur- furlanetto et al found that edi-sf cutoffof gery. recent rbi produced highest myocardial infarction month value. index infarction. an optimal our study designated was reported when major minor also allowed detection ofall depression. were considered. higher studies. false-positive rates we observed many nondepressed identied depressed is probably due ourfocus only. by means bdi-sf. diagnosis. again somewhat lower o1 cognitive-only instruments hospitalized theory. used discrepancy between measure types ofdepres- those earlier report may be different sion affective. behavioral populations. compared general should more accurate detecting depres- patients. surgical about discharged are only from had blunting camgbdiii hamilton rating scale area under curve="0.968" ci p d.0- o.e specificity total _cutoff d.b d.2 receiver-operating-characteristic curves discharge. threshold diagnosis low medians interquartile ranges multimodal bdi observed. population median whereas thresholds required cogni- bdi-sf score tive bdi- scored thus pc used. although further needed confirm these findings presence postopera- problems relatively tively generated ensure screen- explain ing bdi. conversely case reports omission moderately yield influence diverse auc .85 .87. so level nonetheless recommended associated sensitivities cutoffs previously recommended. limitations suspect characteristics several limitations. first depressive studied not gener- surgery must differ some way alizable men mixed samples women. second sample size small. deter- considered mination roc analysis depends who seem require interobserver accuracy aicc tournal critical cart volume www.ajcconline.org scanned camscannertable discriminative discharge months positive misclassification false-negative overall: w screening: wo diagnosis: n un no co ratio ideal would adequacy supported use observer make diagnostic determina- chance missing undergone tions eliminating error coronary artery ation minimized. truly finding prevalence recog- bypass graft similar preva- nized receive in- lence studies cardiac depth therefore been sufficient if purpose testing streamline addition differences enhance recognition nonde- then pressed might identified because small vulner- important. able type ii error. however example larger include proportion observer-rated important requires rater assess generalizability responses specific items. there- across like- fore time wise refinement points training does relevance against sociodemographic settings which strata valuable. limit its shorter forms rea- significance sonable alternatives. self-report pilot data cau- usually take less minutes complete tiously drawing inferences practice they clinically significant testing. but still cygrow.afcconline.org camscanner ncc journal given table note doering l gerard magsarili m cowan m. differed surgery: just blues circus lation. accepted cutoffs. kessler rc mcgonagle ka zhao s al. lifetime warranted dsm-iii-r psychiatric disorders united states: results national comorbidity evaluate appropriate vey. arch gen psychiatry. dunlop dd song j lyons js manheim lm chang rw. racial among pre- etirement adults. am public health. conclusion- heart association. disease stroke statistics: update. dallas tex: asso- provide initial support ciation baker ra andrew mu schrader g knight jl. preoperative bdi-pc test gery: preliminary findings. anz surg. surgery. saur cd granger bb mulbaier lh symp- toms outcome grafting. purposes crit care. diagnoses recom- scheier mf matthews owens jf optimism rehospitalization mended consid intern med. ered berglund demler epidemiology disorder: variety survey replication jama. gottlieb ss khatta friedmann age gender race failure coll cardiol. mendes de leon c dilillo v czajkowski psychoso- little cial acute infarction: enrichd study. enhancing recovery disease. cardiopulmonaryl. helpful diag- anderson rj freedland ke clouse re lustman pj. nosis. sam- comorbid diabetes: meta-analysis. diabetes ples rich mw skala ja warranted. congestive failure. psychosom carandang jm franco-bronson k kamarei s. recognizing financial disclosures managing throughout stages this grants nimh k01mh01700 life. cleve clin r01nr009228 institute mental carney rm interview structured rationale devel opment validity. miller pr dasher r collins griffiths brown f. inpatient eletters assessments i: vs now you read article create contribute unstructured interviews. psychiatry res. online discussion topic using eletters. richter werner heerlein kraus sauer h. visit click validity inventory: review. psy- either full-text .pdf view article. hopathology. mendlowicz mv romildo bueno j. inventory-short moderate references severe inpatients. affect dis. . ke. med- ical morbidity biol steer cavalieri ta leonard dm at. screen frasure-smith lesperance disorders. hosp chological risks following endicott cohen nee fleiss sarantakos burker ej blumenthal feldman scale: extracted regular male female undergoing br change versions schedule psychol. schizophrenia. mckhann gm borowicz goldsborough ma enger state therapy: selnes oa. decline retrospective. lancet. tombaugh tn mcintyre nj. mini-mental exami- pirraglia peterson williams-russok gorkin charl- nation: comprehensive geriatroc. son symptomatology int geriatresychiatry. joray wietlisbach bula cj. impairment elderly inpatients: six- mccrone lenz tarzian perkins anxiety outcomes. geriatraychiatry. depression: incidence patterns coro- ge stetler ca banks wa nary appl nurs pathways linking adiposity inflammatory markers healthy young brain behav immun connerney shapiro pa mclaughlin bagiella sloan rp. relation r. manual. san outcome: prospective antonio psychological corp psychometric properties iournal>