

Answered step by step
Verified Expert Solution
Question
1 Approved Answer
chapter 15 15.7 assignment following are the fig.15.7 and fig.15.6 ASSIGNMENT 15.7 PROOFREAD A COMPUTER-GENERATED HEALTH INSURANCE CLAIM FORM AND LOCATE INCORRECT AND MISSING DATA
chapter 15 15.7 assignment
following are the fig.15.7 and fig.15.6
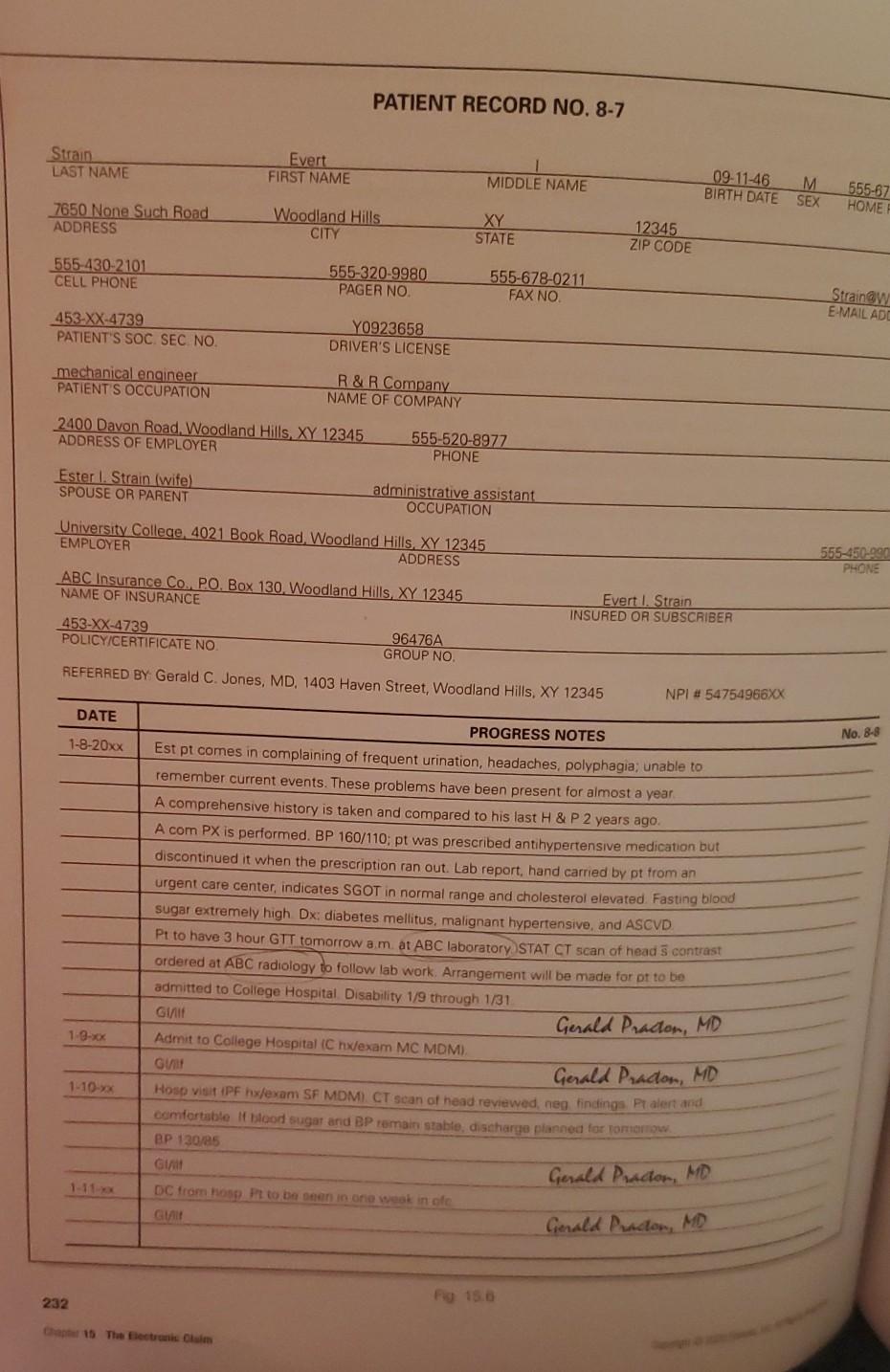
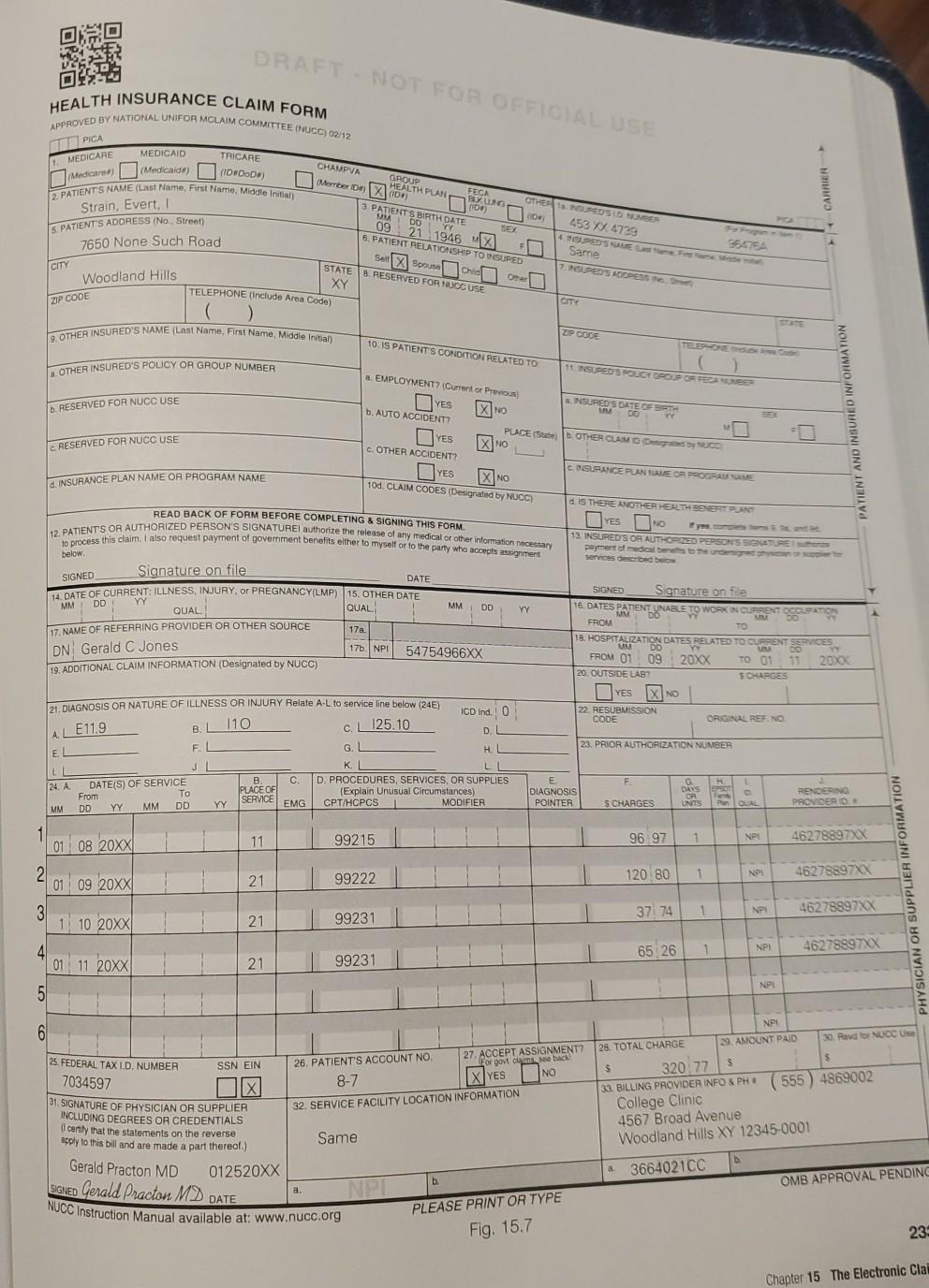
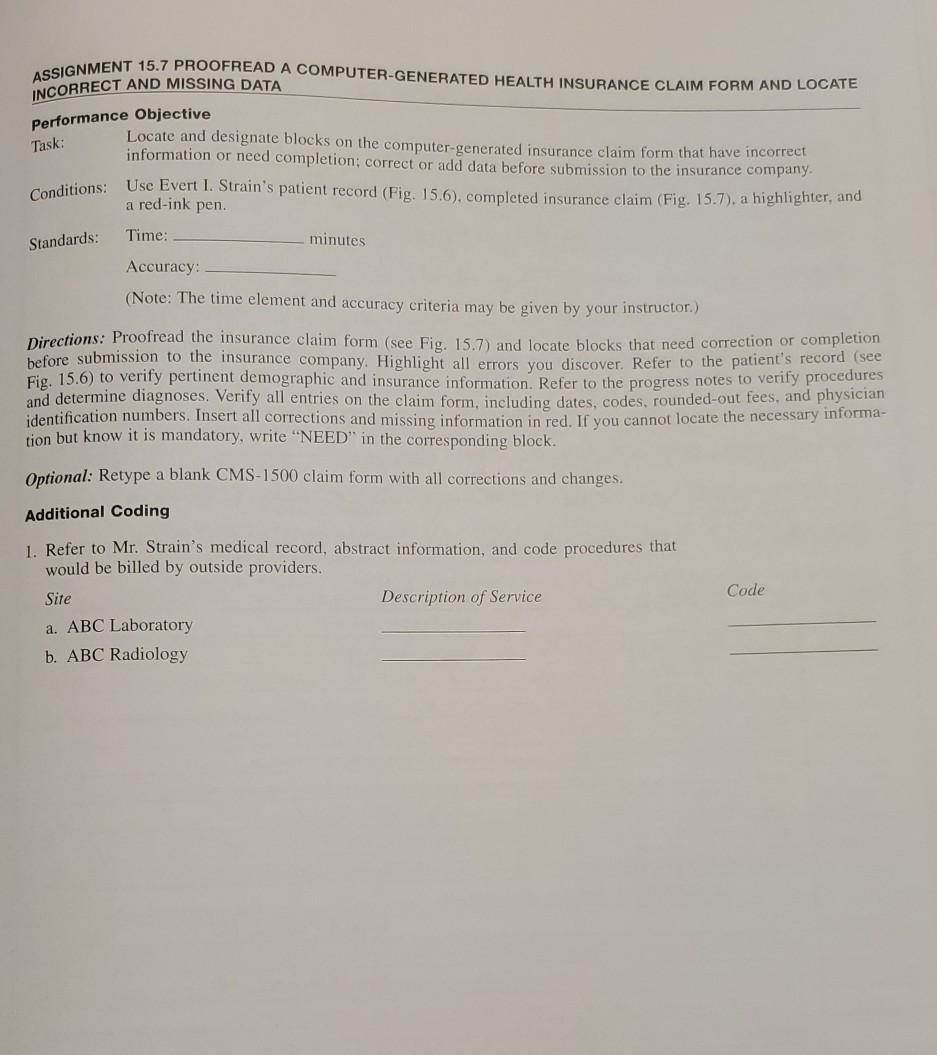
ASSIGNMENT 15.7 PROOFREAD A COMPUTER-GENERATED HEALTH INSURANCE CLAIM FORM AND LOCATE INCORRECT AND MISSING DATA Performance Objective Task: Locate and designate blocks on the computer-generated insurance claim form that have incorrect information or need completion; correct or add data before submission to the insurance company. Condition: Use Evert I. Strain's patient record (Fig. 15.6), completed insurance claim (Fig. 15.7), a highlighter, and a red-ink pen. Standards: Time: minutes Accuracy: (Note: The time element and accuracy criteria may be given by your instructor) Directions: Proofread the insurance claim form (see Fig. 15.7) and locate blocks that need correction or completion before submission to the insurance company. Highlight all errors you discover. Refer to the patient's record (see Fig. 15.6) to verify pertinent demographic and insurance information. Refer to the progress notes to verify procedures and determine diagnoses. Verify all entries on the claim form, including dates, codes, rounded-out fees, and physician identification numbers. Insert all corrections and missing information in red. If you cannot locate the necessary informa- tion but know it is mandatory, write "NEED" in the corresponding block. Optional: Retype a blank CMS-1500 claim form with all corrections and changes. Additional Coding Code 1. Refer to Mr. Strain's medical record, abstract information, and code procedures that would be billed by outside providers. Site Description of Service a. ABC Laboratory b. ABC Radiology PATIENT RECORD NO. 8-7 Strain LAST NAME Evert FIRST NAME MIDDLE NAME 09-11-46 BIRTH DATE M SEX 555-67 HOME 7650 None Such Road ADDRESS Woodland Hills CITY XY STATE 12345 ZIP CODE 555 430-2101 CELL PHONE 555-320-9980 PAGER NO. 555-678-0211 FAX NO Strainaw E-MAIL ADD 453-XX-4739 PATIENT'S SOC. SEC NO. Y0923658 DRIVER'S LICENSE mechanical engineer PATIENT S OCCUPATION R & R Company NAME OF COMPANY 2400 Davon Road, Woodland Hills XY 12345 ADDRESS OF EMPLOYER 555-520-8977 PHONE Ester 1 Strain (wife) SPOUSE OR PARENT administrative assistant OCCUPATION University College 4021 Book Road, Woodland Hills XY 12345 EMPLOYER ADDRESS 555-450-990 PHONE ABC Insurance Co. PO, Box 130. Woodland Hills, XY 12345 NAME OF INSURANCE Evert I. Strain INSURED OR SUBSCRIBER 453-XX-4739 POLICY/CERTIFICATE NO. 96476A GROUP NO REFERRED BY Gerald C. Jones, MD, 1403 Haven Street, Woodland Hills, XY 12345 NPI # 54754966XX DATE No. 8-8 1-8-20xx PROGRESS NOTES Est pt comes in complaining of frequent urination, headaches, polyphagia: unable to remember current events. These problems have been present for almost a year A comprehensive history is taken and compared to his last H & P 2 years ago A com PX is performed. BP 160/110; pt was prescribed antihypertensive medication but discontinued it when the prescription ran out. Lab report, hand carried by pt from an urgent care center indicates SGOT in normal range and cholesterol elevated. Fasting blood sugar extremely high Dx diabetes mellitus, malignant hypertensive, and ASCVD. Pt to have 3 hour GTT tomorrow am at ABC laboratory STAT CT scan of head 5 contrast ordered at ABC radiology to follow lab work. Arrangement will be made for pt to be admitted to College Hospital Disability 1/9 through 1/31 Girlf Gerald Practon, MD Admit to College Hospital (C hx/exam MC MDM), GV Gerald Prador, MD Hoso visit IPF hxlexam SF MDM) CT scan of head reviewed, neg findings Palert and comfortable it blood sugar and BP remain stable, discharge planned for for BP 130/85 Git DC from hosp Pt to be seen in one wok in of GIA Gerald Pader, MD 1-9-xx 1-10- Gerald Peador, MD 232 15 The Electronicam DRAFT NOT FOR OFFICIAL USE HEALTH INSURANCE CLAIM FORM APPROVED BY NATIONAL UNIFOR MCLAIM COMMITTEE NUCC) 02/12 TRICARE TIPICA MEDICARE Medicare) MEDICAID (Medicaide (01000) 2 PATIENTS NAME (Last Name, First Name, Middle Initial) CARRIER Strain, Evert, 5. PATIENTS ADORESS (No. Street) CHAMPVA GROUP FECA HEALTH PLAN BUG OTHER SUPEUS DONES Mermber (10) 10 452 X 4738 3 PATIENTS BIRTH DATE WA DO 4 SUPED SELF- 09 21 1946 Sarne 6. PATIENT RELATIONSHIP TO SUPED Sell X Spo Or STATE 8 RESERVED FOR TOUCC USE XY ZIP CODE 7650 None Such Road CITY ourn Woodland Hills ZIP CODE TELEPHONE (include Area Code) ( 9. OTHER INSURED'S NAME (Last Name, First Name Middle Initial) 10. IS PATIENTS CONDITION RELATED TO a OTHER INSURED'S POLICY OR GROUP NUMBER 1 SUPED S POUCT GROUP OR FECUNE RESERVED FOR NUCC USE EMPLOYMENT? (Current or Prerow INSURED S DATE OFERT OF YES X NO b. AUTO ACCIDENT? PLACE State) OTHER CLASS OBUD YES XNO c. OTHER ACCIDENT? CASURANCE PUNE OR POGUE YES 10d. CLAIM CODES (Designated by NUCC) d. IS THERE ANOTHER HEALTH BENT res No READ BACK OF FORM BEFORE COMPLETING & SIGNING THIS FORM. 13. INSUREDS OR AUTHOPED PERSONS SILATURI PATIENT AND INSURED INFORMATION RESERVED FOR NUCC USE INSURANCE PLAN NAME OA PROGRAM NAME X NO 12. PATIENTS OR AUTHORIZED PERSON'S SIGNATUREI authorize the release of any medical or other information necessary to process this claim. I also request payment of government benefits either to myself or to the party who accepts assignment below SIGNED DD YY SIGNED Signature on file 16. DATES PATENT UNABLE TO WORK IN CURRENT MM MM DD YY Signature on file DATE 4. DATE OF CURRENT ILLNESS, INJURY OF PREGNANCY(LMP) 15. OTHER DATE QUAL QUAL 17. NAME OF REFERRING PROVIDER OR OTHER SOURCE 17a. DN Gerald C Jones 17. NPI 54754966XX 19. ADDITIONAL CLAIM INFORMATION (Designated by NUCC) FROM 18. HOSPITALIZATION DATES RELATED TO CREATE FROM 01 09 20XX TO 01 11 2030 SCHARGES IX NO 20. OUTSIDE LAB YES 22 RESUBMISSION CODE ORIGINAL REF. NO AL E11.9 23. PRIOR AUTHORIZATION NUMBER 21. DIAGNOSIS OR NATURE OF ILLNESS OR INJURY Relate A-L to service line below (24) ICD Ind. 0 110 B c. 125.10 D. EL F G H LL J K L [24. A DATE(S) OF SERVICE B C. D. PROCEDURES, SERVICES, OR SUPPLIES From To PLACE OF (Explain Unusual Circumstances) SERVICE MM DD YY DD MM YY EMG CPT/HCPCS MODIFIER 1 01 08 20XX 11 99215 F th E DIAGNOSIS POINTER G DAYS UNITS RENDERING PROVIDERD S CHARGES POUL 96 97 1 1 NPI 46278897XX 1 120 80 NP 46278897XX 21 99222 2 01 09 20XX 3 1 10 20XX SUPPLIERI NP 1 37 74 46278897% 21 99231 65 26 1 NPI 46278897% 21 99231 4 01 11 20XX 5 NPI 6 26. PATIENT'S ACCOUNT NO 27. ACCEPT ASSIGNMENT? For govt 30 8-7 IX YES NO 32. SERVICE FACILITY LOCATION INFORMATION 25. FEDERAL TAX LD NUMBER SSN EIN 7034597 X SIGNATURE OF PHYSICIAN OR SUPPLIER INCLUDING DEGREES OR CREDENTIALS certify that the statements on the reverse apply to this bill and are made a part thereat.) Gerald Practon MD 012520XX SIGNED Gerald Practon MD DATE NUCC Instruction Manual available at: www.nucc.org NPE 28. TOTAL CHARGE 29. AMOUNT PAID 30. Raval NUCCU $ 320.77 3 $ 33 BILLING PROVIDER INFO & PH 555 ) 4869002 College Clinic 4567 Broad Avenue Woodland Hills XY 12345-0001 Same a 3664021CC b OMB APPROVAL PENDING a NPT PLEASE PRINT OR TYPE Fig. 15.7 23 Chapter 15 The Electronic Cla ASSIGNMENT 15.7 PROOFREAD A COMPUTER-GENERATED HEALTH INSURANCE CLAIM FORM AND LOCATE INCORRECT AND MISSING DATA Performance Objective Task: Locate and designate blocks on the computer-generated insurance claim form that have incorrect information or need completion; correct or add data before submission to the insurance company. Condition: Use Evert I. Strain's patient record (Fig. 15.6), completed insurance claim (Fig. 15.7), a highlighter, and a red-ink pen. Standards: Time: minutes Accuracy: (Note: The time element and accuracy criteria may be given by your instructor) Directions: Proofread the insurance claim form (see Fig. 15.7) and locate blocks that need correction or completion before submission to the insurance company. Highlight all errors you discover. Refer to the patient's record (see Fig. 15.6) to verify pertinent demographic and insurance information. Refer to the progress notes to verify procedures and determine diagnoses. Verify all entries on the claim form, including dates, codes, rounded-out fees, and physician identification numbers. Insert all corrections and missing information in red. If you cannot locate the necessary informa- tion but know it is mandatory, write "NEED" in the corresponding block. Optional: Retype a blank CMS-1500 claim form with all corrections and changes. Additional Coding Code 1. Refer to Mr. Strain's medical record, abstract information, and code procedures that would be billed by outside providers. Site Description of Service a. ABC Laboratory b. ABC Radiology PATIENT RECORD NO. 8-7 Strain LAST NAME Evert FIRST NAME MIDDLE NAME 09-11-46 BIRTH DATE M SEX 555-67 HOME 7650 None Such Road ADDRESS Woodland Hills CITY XY STATE 12345 ZIP CODE 555 430-2101 CELL PHONE 555-320-9980 PAGER NO. 555-678-0211 FAX NO Strainaw E-MAIL ADD 453-XX-4739 PATIENT'S SOC. SEC NO. Y0923658 DRIVER'S LICENSE mechanical engineer PATIENT S OCCUPATION R & R Company NAME OF COMPANY 2400 Davon Road, Woodland Hills XY 12345 ADDRESS OF EMPLOYER 555-520-8977 PHONE Ester 1 Strain (wife) SPOUSE OR PARENT administrative assistant OCCUPATION University College 4021 Book Road, Woodland Hills XY 12345 EMPLOYER ADDRESS 555-450-990 PHONE ABC Insurance Co. PO, Box 130. Woodland Hills, XY 12345 NAME OF INSURANCE Evert I. Strain INSURED OR SUBSCRIBER 453-XX-4739 POLICY/CERTIFICATE NO. 96476A GROUP NO REFERRED BY Gerald C. Jones, MD, 1403 Haven Street, Woodland Hills, XY 12345 NPI # 54754966XX DATE No. 8-8 1-8-20xx PROGRESS NOTES Est pt comes in complaining of frequent urination, headaches, polyphagia: unable to remember current events. These problems have been present for almost a year A comprehensive history is taken and compared to his last H & P 2 years ago A com PX is performed. BP 160/110; pt was prescribed antihypertensive medication but discontinued it when the prescription ran out. Lab report, hand carried by pt from an urgent care center indicates SGOT in normal range and cholesterol elevated. Fasting blood sugar extremely high Dx diabetes mellitus, malignant hypertensive, and ASCVD. Pt to have 3 hour GTT tomorrow am at ABC laboratory STAT CT scan of head 5 contrast ordered at ABC radiology to follow lab work. Arrangement will be made for pt to be admitted to College Hospital Disability 1/9 through 1/31 Girlf Gerald Practon, MD Admit to College Hospital (C hx/exam MC MDM), GV Gerald Prador, MD Hoso visit IPF hxlexam SF MDM) CT scan of head reviewed, neg findings Palert and comfortable it blood sugar and BP remain stable, discharge planned for for BP 130/85 Git DC from hosp Pt to be seen in one wok in of GIA Gerald Pader, MD 1-9-xx 1-10- Gerald Peador, MD 232 15 The Electronicam DRAFT NOT FOR OFFICIAL USE HEALTH INSURANCE CLAIM FORM APPROVED BY NATIONAL UNIFOR MCLAIM COMMITTEE NUCC) 02/12 TRICARE TIPICA MEDICARE Medicare) MEDICAID (Medicaide (01000) 2 PATIENTS NAME (Last Name, First Name, Middle Initial) CARRIER Strain, Evert, 5. PATIENTS ADORESS (No. Street) CHAMPVA GROUP FECA HEALTH PLAN BUG OTHER SUPEUS DONES Mermber (10) 10 452 X 4738 3 PATIENTS BIRTH DATE WA DO 4 SUPED SELF- 09 21 1946 Sarne 6. PATIENT RELATIONSHIP TO SUPED Sell X Spo Or STATE 8 RESERVED FOR TOUCC USE XY ZIP CODE 7650 None Such Road CITY ourn Woodland Hills ZIP CODE TELEPHONE (include Area Code) ( 9. OTHER INSURED'S NAME (Last Name, First Name Middle Initial) 10. IS PATIENTS CONDITION RELATED TO a OTHER INSURED'S POLICY OR GROUP NUMBER 1 SUPED S POUCT GROUP OR FECUNE RESERVED FOR NUCC USE EMPLOYMENT? (Current or Prerow INSURED S DATE OFERT OF YES X NO b. AUTO ACCIDENT? PLACE State) OTHER CLASS OBUD YES XNO c. OTHER ACCIDENT? CASURANCE PUNE OR POGUE YES 10d. CLAIM CODES (Designated by NUCC) d. IS THERE ANOTHER HEALTH BENT res No READ BACK OF FORM BEFORE COMPLETING & SIGNING THIS FORM. 13. INSUREDS OR AUTHOPED PERSONS SILATURI PATIENT AND INSURED INFORMATION RESERVED FOR NUCC USE INSURANCE PLAN NAME OA PROGRAM NAME X NO 12. PATIENTS OR AUTHORIZED PERSON'S SIGNATUREI authorize the release of any medical or other information necessary to process this claim. I also request payment of government benefits either to myself or to the party who accepts assignment below SIGNED DD YY SIGNED Signature on file 16. DATES PATENT UNABLE TO WORK IN CURRENT MM MM DD YY Signature on file DATE 4. DATE OF CURRENT ILLNESS, INJURY OF PREGNANCY(LMP) 15. OTHER DATE QUAL QUAL 17. NAME OF REFERRING PROVIDER OR OTHER SOURCE 17a. DN Gerald C Jones 17. NPI 54754966XX 19. ADDITIONAL CLAIM INFORMATION (Designated by NUCC) FROM 18. HOSPITALIZATION DATES RELATED TO CREATE FROM 01 09 20XX TO 01 11 2030 SCHARGES IX NO 20. OUTSIDE LAB YES 22 RESUBMISSION CODE ORIGINAL REF. NO AL E11.9 23. PRIOR AUTHORIZATION NUMBER 21. DIAGNOSIS OR NATURE OF ILLNESS OR INJURY Relate A-L to service line below (24) ICD Ind. 0 110 B c. 125.10 D. EL F G H LL J K L [24. A DATE(S) OF SERVICE B C. D. PROCEDURES, SERVICES, OR SUPPLIES From To PLACE OF (Explain Unusual Circumstances) SERVICE MM DD YY DD MM YY EMG CPT/HCPCS MODIFIER 1 01 08 20XX 11 99215 F th E DIAGNOSIS POINTER G DAYS UNITS RENDERING PROVIDERD S CHARGES POUL 96 97 1 1 NPI 46278897XX 1 120 80 NP 46278897XX 21 99222 2 01 09 20XX 3 1 10 20XX SUPPLIERI NP 1 37 74 46278897% 21 99231 65 26 1 NPI 46278897% 21 99231 4 01 11 20XX 5 NPI 6 26. PATIENT'S ACCOUNT NO 27. ACCEPT ASSIGNMENT? For govt 30 8-7 IX YES NO 32. SERVICE FACILITY LOCATION INFORMATION 25. FEDERAL TAX LD NUMBER SSN EIN 7034597 X SIGNATURE OF PHYSICIAN OR SUPPLIER INCLUDING DEGREES OR CREDENTIALS certify that the statements on the reverse apply to this bill and are made a part thereat.) Gerald Practon MD 012520XX SIGNED Gerald Practon MD DATE NUCC Instruction Manual available at: www.nucc.org NPE 28. TOTAL CHARGE 29. AMOUNT PAID 30. Raval NUCCU $ 320.77 3 $ 33 BILLING PROVIDER INFO & PH 555 ) 4869002 College Clinic 4567 Broad Avenue Woodland Hills XY 12345-0001 Same a 3664021CC b OMB APPROVAL PENDING a NPT PLEASE PRINT OR TYPE Fig. 15.7 23 Chapter 15 The Electronic Cla
Step by Step Solution
There are 3 Steps involved in it
Step: 1

Get Instant Access to Expert-Tailored Solutions
See step-by-step solutions with expert insights and AI powered tools for academic success
Step: 2

Step: 3
Ace Your Homework with AI
Get the answers you need in no time with our AI-driven, step-by-step assistance
Get Started
Public Finance and Public Policy
Authors: Jonathan Gruber
4th edition
1429278455, 978-1429278454