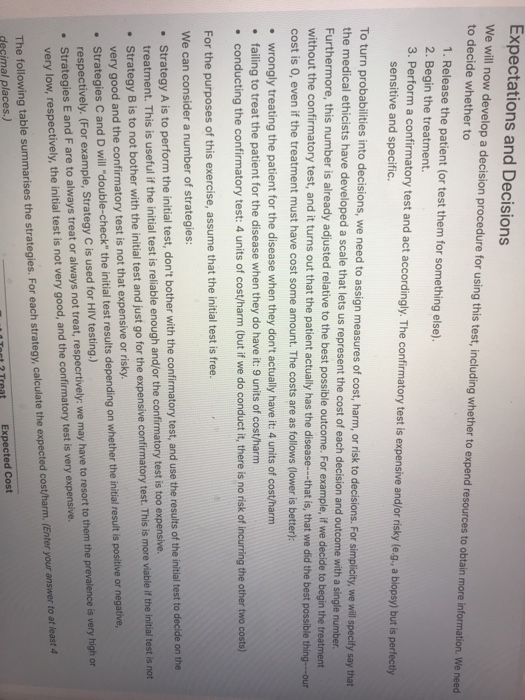
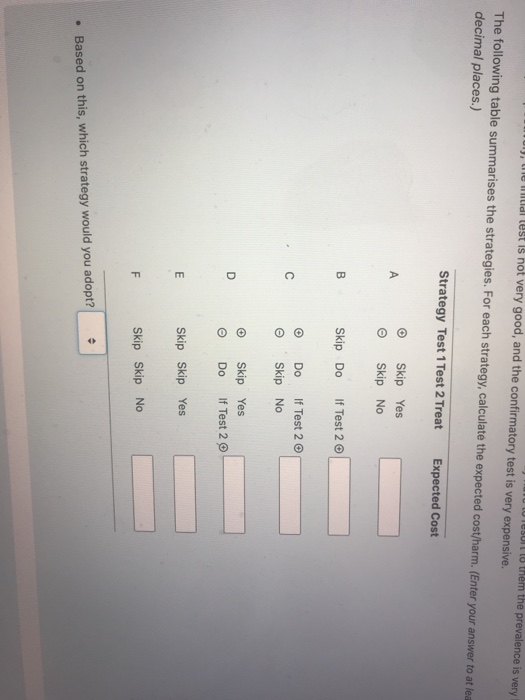
Expectations and Decisions We will now develop a decision procedure for using this test, including whether to expend resources to obtain more information. We need to decide whether to 1. Release the patient (or test them for something else). 2. Begin the treatment. 3. Perform a confirmatory test and act accordingly. The confirmatory test is expensive and/or risky (e.g., a biopsy) but is perfectly sensitive and specific To turn probabilities into decisions, we need to assign measures of cost, harm, or risk to decisions. For simplicity, we will specify say that the medical ethicists have developed a scale that lets us represent the cost of each decision and outcome with a single number. Furthermore, this number is already adjusted relative to the best possible outcome. For example, if we decide to begin the treatment without the confirmatory test, and it turns out that the patient actually has the disease---that is, that we did the best possible thing---our cost is o, even if the treatment must have cost some amount. The costs are as follows (lower is better): wrongly treating the patient for the disease when they don't actually have it: 4 units of cost/harm failing to treat the patient for the disease when they do have it: 9 units of cost/harm conducting the confirmatory test: 4 units of cost/harm (but if we do conduct it, there is no risk of incurring the other two costs) For the purposes of this exercise, assume that the initial test is free. We can consider a number of strategies: Strategy A is to perform the initial test, don't bother with the confirmatory test, and use the results of the initial test to decide on the treatment. This is useful if the initial test is reliable enough and/or the confirmatory test is too expensive. Strategy B is to not bother with the initial test and just go for the expensive confirmatory test. This is more viable if the initial test is not very good and the confirmatory test is not that expensive or risky. Strategies C and D will "double-check" the initial test results depending on whether the initial result is positive or negative, respectively. (For example, Strategy C is used for HIV testing.) Strategies E and F are to always treat or always not treat, respecrtively: we may have to resort to them the prevalence is very high or very low, respectively, the initial test is not very good, and the confirmatory test is very expensive. The following table summarises the strategies. For each strategy, calculate the expected cost/harm. (Enter your answer to at least 4 decimal places.) Expected Cost CSI lo them the prevalence is very ul), le lidl lest is not very good, and the confirmatory test is very expensive. The following table summarises the strategies. For each strategy, calculate the expected cost/harm. (Enter your answer to at lea decimal places.) Strategy Test 1 Test 2 Treat Expected Cost Yes Skip Skip No B Skip Do If Test 2 c Do If Test 2 Skip No O D 0 0 Skip Yes Do If Test 2 ILLI E Skip Skip Yes F Skip Skip No Based on this, which strategy would you adopt? Expectations and Decisions We will now develop a decision procedure for using this test, including whether to expend resources to obtain more information. We need to decide whether to 1. Release the patient (or test them for something else). 2. Begin the treatment. 3. Perform a confirmatory test and act accordingly. The confirmatory test is expensive and/or risky (e.g., a biopsy) but is perfectly sensitive and specific To turn probabilities into decisions, we need to assign measures of cost, harm, or risk to decisions. For simplicity, we will specify say that the medical ethicists have developed a scale that lets us represent the cost of each decision and outcome with a single number. Furthermore, this number is already adjusted relative to the best possible outcome. For example, if we decide to begin the treatment without the confirmatory test, and it turns out that the patient actually has the disease---that is, that we did the best possible thing---our cost is o, even if the treatment must have cost some amount. The costs are as follows (lower is better): wrongly treating the patient for the disease when they don't actually have it: 4 units of cost/harm failing to treat the patient for the disease when they do have it: 9 units of cost/harm conducting the confirmatory test: 4 units of cost/harm (but if we do conduct it, there is no risk of incurring the other two costs) For the purposes of this exercise, assume that the initial test is free. We can consider a number of strategies: Strategy A is to perform the initial test, don't bother with the confirmatory test, and use the results of the initial test to decide on the treatment. This is useful if the initial test is reliable enough and/or the confirmatory test is too expensive. Strategy B is to not bother with the initial test and just go for the expensive confirmatory test. This is more viable if the initial test is not very good and the confirmatory test is not that expensive or risky. Strategies C and D will "double-check" the initial test results depending on whether the initial result is positive or negative, respectively. (For example, Strategy C is used for HIV testing.) Strategies E and F are to always treat or always not treat, respecrtively: we may have to resort to them the prevalence is very high or very low, respectively, the initial test is not very good, and the confirmatory test is very expensive. The following table summarises the strategies. For each strategy, calculate the expected cost/harm. (Enter your answer to at least 4 decimal places.) Expected Cost CSI lo them the prevalence is very ul), le lidl lest is not very good, and the confirmatory test is very expensive. The following table summarises the strategies. For each strategy, calculate the expected cost/harm. (Enter your answer to at lea decimal places.) Strategy Test 1 Test 2 Treat Expected Cost Yes Skip Skip No B Skip Do If Test 2 c Do If Test 2 Skip No O D 0 0 Skip Yes Do If Test 2 ILLI E Skip Skip Yes F Skip Skip No Based on this, which strategy would you adopt