help pls!
CASE STUDY: Strategic Planning in Lesedi District, South Africa
What are the (at least) 3 major issues found in this case study (e.g., mission/vision statement, performance maeasyremwnr, leadership and effective communication, negotiation and conflcit resolution skills, budget and resource allocation)? What are the recommendations to solve them?
Appendix
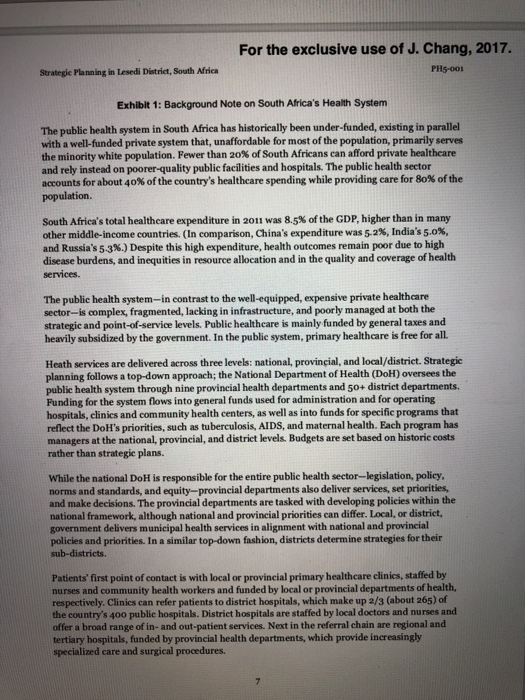
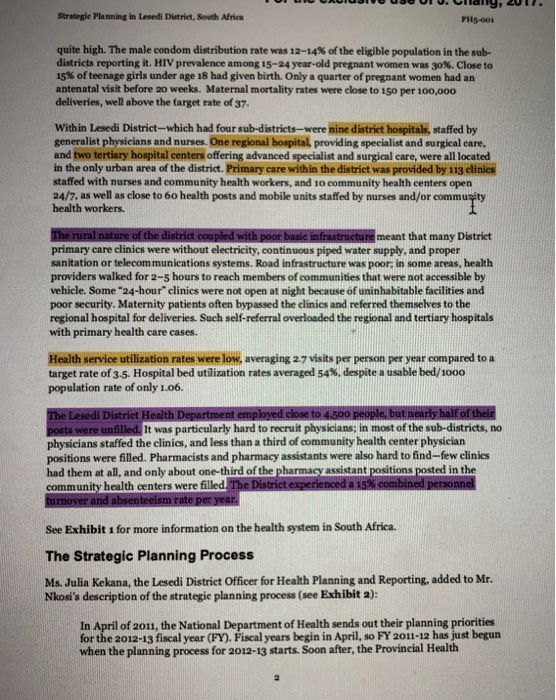
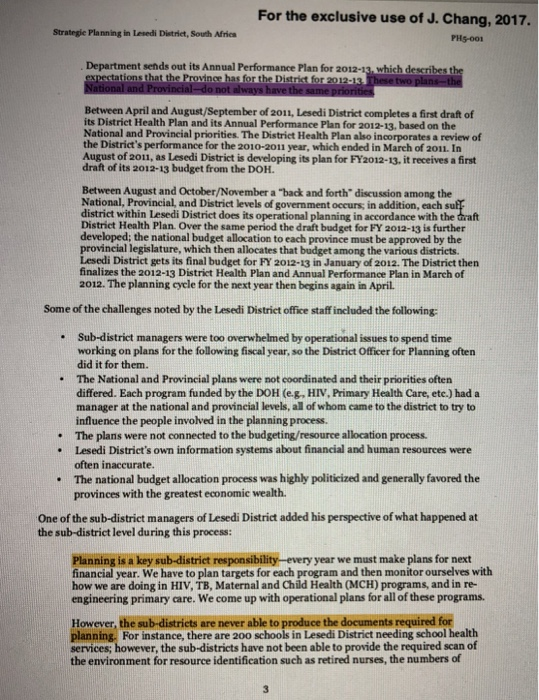
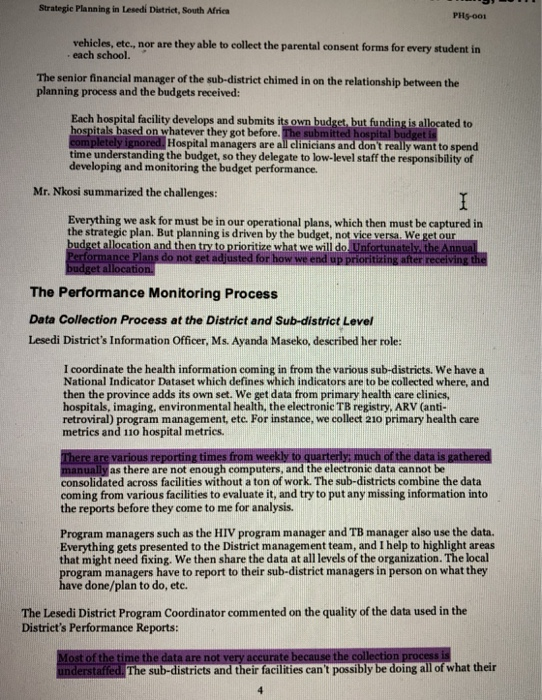
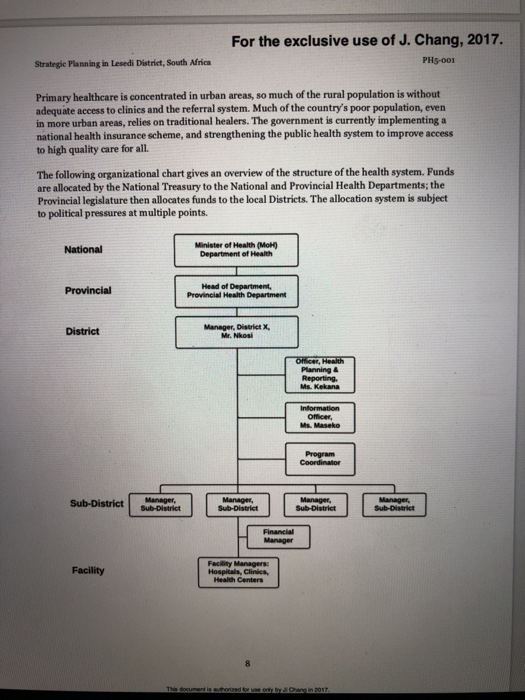
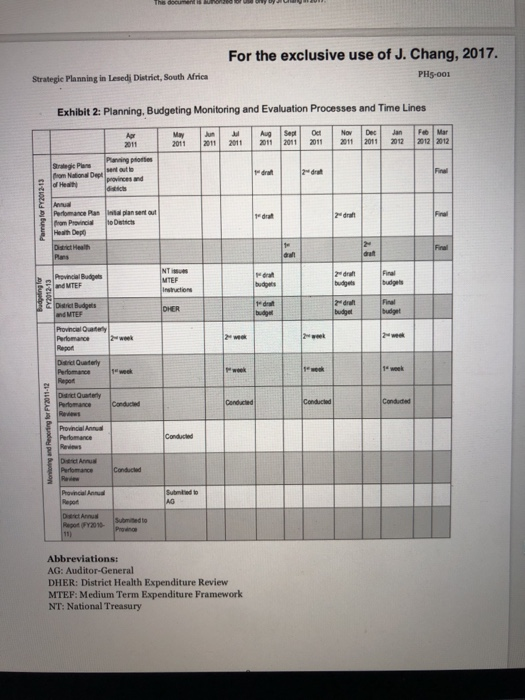
Strategie Planning in Lesedi District, South Africa quite high. The male condom distribution rate was 12-14% of the eligible population in the sub- districts reporting it. HIV prevalence among 15-24 year-old pregnant women was 30%. Close to 15% of teenage girls under age 18 had given birth. Only a quarter of pregnant women had an antenatal visit before 20 weeks. Maternal mortality rates were close to 150 per 100,000 deliveries, well above the farget rate of 37 Within Lesedi District-which had four sub-districts-were nine district hospitals, staffed by generalist physicians and nurses. One regional hospital, providing specialist and surgical care and two tertiary hospital centers offering advanced specialist and surgical care, were all located in the only urban area of the district. Primary care within the district was provided by 113 clinics staffed with nurses and community health workers, and 1o community health centers open 24/7, as well as close to 6o health posts and mobile units staffed by nurses and/or commusity health workers. th poor basic infrastructure meant that many Distriet primary care clinics were without electricity, continuous piped water supply, and proper sanitation or telecommunications systems. Road infrastructure was poor; in some areas, health providers walked for 2-5 hours to reach members of communities that were not accessible by vehicle. Some "24-hour" clinics were not open at night because of uninhabitable facilities and poor security. Maternity patients often bypassed the clinics and referred themselves to the regional hospital for deliveries. Such self-referral overloaded the regional and tertiary hospitals with primary health care cases. Health service utilization rates were low, averaging 27 visits per person per year compared to a target rate of 3.5. Hospital bed utilization rates averaged 54%, despite a usable bed/1000 population rate of only 1.06. ts were unfilled. It was particularly hard to recruit physicians; in most of the sub-districts, no physicians staffed the clinics, and less than a third of community health center physician positions were filled. Pharmacists and pharmacy assistants were also hard to find-few clinics had them at all, and only about one-third of the pharmacy assistant positions posted community health centers were filled in the See Exhibit 1 for more information on the health system in South Africa. The Strategic Planning Process Ms. Julia Kekana, the Lesedi District Officer for Health Planning and Reporting, added to Mr. Nkosi's description of the strategie planning process (see Exhibit a): In April of 2011, the National Department of Health sends out their planning priorities for the 2012-13 fiscal year (FY). Fiscal years begin in April, so FY 2011-12 has just begun when the planning process for 2012-13 starts. Soon after, the Provincial Health 2 Strategie Planning in Lesedi District, South Africa PHS-001 vehicles, etc., nor are they able to eolleet the parental consent forms for every student in . each school. The senior financial manager of the sub-district chimed in on the relationship between the planning process and the budgets received: Each hospital facility develops and submits its own budget, but funding is allocated to hospitals based on whatever they got before. The submitted Hospital managers are all clinicians and don't really want to spend time understanding the budget, so they delegate to low-level staff the responsibility of developing and monitoring the budget performance Mr. Nkosi summarized the challenges Everything we ask for must be in our operational plans, which then must be captured in the strategie plan. But planning is driven by the budget, not vice versa. We get our The Performance Monitoring Process Data Collection Process at the District and Sub-district Level Lesedi District's Information Officer, Ms. Ayanda Maseko, described her role: I coordinate the health information coming in from the various sub-districts. We have a National Indicator Dataset which defines which indicators are to be collected where, and then the province adds its own set. We get data from primary health care clinics, hospitals, imaging, environmental health, the electronic TB registry, ARV (anti- retroviral) program management, ete. For instance, we collect 210 primary health care metrics and 110 hospital metrics. as there are not enough computers, and the electronic data cannot be consolidated across facilities without a ton of work. The sub-districts combine the data coming from various facilities to evaluate it, and try to put any missing information into the reports before they come to me for analysis. Program managers such as the HIV program manager and TB manager also use the data. Everything gets presented to the District management team, and I help to highlight areas that might need fixing. We then share the data at all levels of the organization. The local ram managers have to report to their sub-district managers in person on what they ve done/plan to do, etc. The Lesedi District Program Coordinator commented on the quality of the data used in the District's Performance Reports: The sub-distriets and their facilities can't possibly be doing all of what their l thhe exciusive use ord.Chang, 2017. Strategic Planning in Lesedi District, South Africa PH5-001 reports say they are doing. The original source at clinic will say a number is 4; but in the report, that number is 10. The people producing some of the raw data d hey may not understand what a "midnight census" is-a 8 s such as a "half-day patient. And there is no way to figure out what is wrong we don't have the resources to audit everything so the data is wrong every day. It often undercounts the patient load which then throws the cost estimates off. For instance, a patient sitting in an outpatient clinic all day needs food but isn't counted. Quarterly Performance Reports and Reviews Each sub-district manager reported their data to the District Manager, who, after reviewing it with the sub-district managers, produced a District-wide Department for the Provincial Health i District was required to pril, July, October, and January These reports were generally delivered in person by District Managers to the Provincial office, and their performance was reviewed with provincial leadership. The Province then combined the various District reports and submitted them to the National DOH, generally within a week after receiving the Districts' reports. Mr. Nkosi described the challenge of generating the quarterly reports and undertaking the reviews with his sub-district managers: The quarterly performance meetings with my sub-district and facility managers are not always up to the standards we wish they were. They are often used by the sub-distriet and facility managers as an opportunity to ask for more resources to offset their poor management skills. uns ate When you look below districts a programs to institutions and facilities, there is little clarity regarding what people are supposed to do. For instance, if reducing outpatient employee head count is an objective, you would expect that the hospital CEO would translate that down into the nursing executive's job description, but the linkages are not fully working. And the nursing service manager may not understand how this will impact quality of service for patients. Waiting time reduction is a goal-and there is an expectation that the facility manager will figure out ways to do that, such as having a triage person or a booking system for chronic patients. It is this level of translation, however, that does not always happen. Front-line managers, most of whom are clinicians, need training; people are in these positions in administration for reasons other than administrative skills At the provincial level, other frustrations with the planning and budgeting process emerged. As the Provincial Head of Department (HOD), explained, Department of Health lacks strategie focus We are so busy following the planning e deadlines-and we don't miss the deadlines-that we have to overwork ou this adversely affects productivity, quality of planning and service and long-term budgeting. Finally, we need to synchronize all the different reports livery. Also our trad we need short-, medium-, For the exclusive use of J. Chang, 2017. Strategic Planning in Lesedi District, South Africa PH5-001 We need to train the District Managers and the Provincial executive team to stop pushing paper. The Provincial focus is too operational. We miss the Big Picture. We should let facility managers be operational. We should expect the District Managers in areas with high HIV to ask, "What is it that we are doing wrong and what can we do about it?" And then the budget should move toward HIV, but that is not reflected in the traditional budgeting process. Looking Ahead As District Manager, Mr. Nkosi was hopeful that the future would bring increased resources and better health to his local population. It was imperative that the planning and budgeting process support a healthier future in the district. He was wondering what additional skills he needed to learn to better work the system. He also was thinking about whether the system itself might be improved, and if so, how. For the exclusive use of J. Chang, 2017. PHS-001 Strategic Planning in Lesedi District, South Africa Primary healthcare is concentrated in urban areas, so much of the rural population is without adequate access to elinics and the referral system. Much of the country's poor population, even in more urban areas, relies on traditional healers. The government is currently implementing a national health insurance scheme, and strenthening the public health system to improve access to high quality care for all. The following organizational chart gives an overview of the structure of the health system. Funds are allocated by the National Treasury to the National and Provincial Health Departments; the Provincial legislature then allocates funds to the local Districts. The allocation system is subject to political pressures at multiple points National Minister of Health (MOH) Department of Health Head of Department Provincial Health Department Provincial District Manager, District X. Mr. Nkosi Ms. Kekana Officer, Ms. Maseko Program Coordinator Sub-District ManrMarnages Sub-District Sub-District Manager Facility Health Centers For the exclusive use of J. Chang, 2017. PHs-001 Strategie Planning in Lesedj District, South Africa Exhibit 2: Planning, Budgeting Monitoring and Evaluation Processes and Time Lines 2011 2011 20111011 20112 2 2011 2012 2012 2012 Panning p oes Final am National Dept provinces and dra ram Provincia Health Dept oDisticts Final budgets DHER Provincial Oately te week Pertomance Conducted Promance Conducte Submlied to pot (PY201 Abbreviations: AG: Auditor-General DHER: District Health Expenditure Review MTEF: Medium Term Expenditure Framework NT: National Treasury This dooument is authortzed for use only by Chang in 2017 For the exclusive use of J. Chang, 2017. Strategic Planning in Lesedi District, South Africa PH5-001 Exhibit 2, continued Technical Support Month April to JuneDistrict to review Audit of previous Activities Technical review done for each year's activities (situational analysis district: together with all quarterly reports) DHER and Annual Report Review Tools: .i. District Annual Report .i. District Heath Expenditure Integrity of analysis and Integrity of data sources to be verified Review conclusions veified Confirmation of Provincial Strategic Part A: Identification of challenges Priorities and systems gaps . Prioritisation . First draft District Health Plan for the Part B September forthcoming financial year Results based planning-technical . To be based upon Annual Report and support National and Provincial Priorities First draft of the Provincial Annual Performance for the forthcoming financial year (Inputs from the DHP form the basis for the Programme 2 nputs) .Financial review and financial forecasting-using the DHER as basis-to inform the first submission of Budget statement 2 Interpretation and strategic guidance-new policy directive- .First Draft of MTEF Budget-Budgetimplications and costing Statement 2 (Inputs from the DHER Costing of plans-technical review and the DHP forms the basis for theMarginal adjustments to budgets Programme 2 input) October to National and Provincial MTEC December Hearing and targets Full technical review of District Plans and feedback . 22nd Draft District Health Plarn 2" Draft Provincial Annual Performance Plan 2" Draft Budget Statement 2 January toFinal Budget Allocation Letter Technical support for alignment of plan with confirmed budget Technical support for the operationalization of DHP March Final APP Final DHP This dooument is authorized for use orly by Ji Chang in 2017 For the exclusive use of J. Chang, 2017. Strategic Planning in Lesedi District, South Africa PHs-001 Exhibit 3: National Health Systems Priorities for 2010-2015 Sample District Activities 2015 Facilitate career exhibitions on 2015 Target 85 schools National Priority Provision of Strategic Leadership and Creation of Social Compact for Better Health Outcomes health at high schools Recruit students to study medicine in 7 students Cuba Facilitate access to internal bursary 115 students Conduct Primary Health Care I implement NH Master Plan 16 campaigns Implementation of National Health Insurance Improve the Quality of Heath Assess the implementation of Quality 12 hospitals &10 Services Improvement Plans CHCs Facilitate implementation of Quality Assurance Program Facilitate the reduction of the vacancy rate for critical and scarce skills 160 programs Reduce from 58% to | 45% Train Community Health Workers on 324 workers Reengineering of PHC Revitalization of Infrastructure Urgent implementation of refurbishment and maintenance of district hospitals, CHCs, and Clinics 162 facilities Accelerated Implementation of Implement adult and paediatric HIVIAIDS strategic plan and treatment guidelines at al PHC increased focus on TB and other communicable diseases Mass mobilization for the better health of the population Place more focus on programs to facilities Intensify health promotion programs 16 programs attain Millennium Development Goals Conduct awareness campaigns on diseases of Ifestyle No related District activities Commission research to accurately quantify maternal and infant mortality Commission research on the impact of social determinants of health Review of Drug Policy Strengthen research and For the exclusive use of J. Chang, 2017. PIIs-00r Strategie Planning in Lesedi District, South Africa Exhibit 4: Sample of District Health Plan for Primary Health Care Strategie Goal o1: To facilitate a functional quality-driven primary health care system that provides an integrated and seamless package of health needs, services and is responsive to eustomer Strategic Challenges: Underutilization of PHC due to bad roads, small facilities; poor drug management at all levels; shortage of personnel, inadequate professional skills; poor maintenance systems; lack of sustainable transport; and poor data quality. Measures of Performance: 10 measures of vacancy rates for skilled professionals (doctors, nurses, pharmacists) 5 measures of vacancy rates for other human resource categories at primary health care facilities 15 measures of patient head count, utilization rates, expenditures per head count, and clinical workload per professional nurse and doctor, and facility supervisory visits Exhibit 5: Budget of Lesedi District, 2011-2012 Values in SA Rand Sub Program Provincial Budget %Over Variation from Appropriation Expenditure (Under) Spent Prior Year in Real Terms (5%) 100,247,478 341,030,680 (10%) (3%) 1 10% 90,015,661 330,803,880 District Management Community Health Other Community HMIAIDS 34252.021147380418 25% (68%) 126% 51% 18% 13% 14% 6% 461,663 82,348.286 9,855,834 490,756 71,321,205 (13%) 8,127,845| (18%)| 1 654.864.794 640,198.83 Subtotal: Primary Health Services District Hospitals Total Lesedi District (2%) 12% 3% 616,630,662 689,110.193 1,371,742,934 1,419,322,689 Thie document is authorized lor use orly by Chang in 2017 Strategie Planning in Lesedi District, South Africa quite high. The male condom distribution rate was 12-14% of the eligible population in the sub- districts reporting it. HIV prevalence among 15-24 year-old pregnant women was 30%. Close to 15% of teenage girls under age 18 had given birth. Only a quarter of pregnant women had an antenatal visit before 20 weeks. Maternal mortality rates were close to 150 per 100,000 deliveries, well above the farget rate of 37 Within Lesedi District-which had four sub-districts-were nine district hospitals, staffed by generalist physicians and nurses. One regional hospital, providing specialist and surgical care and two tertiary hospital centers offering advanced specialist and surgical care, were all located in the only urban area of the district. Primary care within the district was provided by 113 clinics staffed with nurses and community health workers, and 1o community health centers open 24/7, as well as close to 6o health posts and mobile units staffed by nurses and/or commusity health workers. th poor basic infrastructure meant that many Distriet primary care clinics were without electricity, continuous piped water supply, and proper sanitation or telecommunications systems. Road infrastructure was poor; in some areas, health providers walked for 2-5 hours to reach members of communities that were not accessible by vehicle. Some "24-hour" clinics were not open at night because of uninhabitable facilities and poor security. Maternity patients often bypassed the clinics and referred themselves to the regional hospital for deliveries. Such self-referral overloaded the regional and tertiary hospitals with primary health care cases. Health service utilization rates were low, averaging 27 visits per person per year compared to a target rate of 3.5. Hospital bed utilization rates averaged 54%, despite a usable bed/1000 population rate of only 1.06. ts were unfilled. It was particularly hard to recruit physicians; in most of the sub-districts, no physicians staffed the clinics, and less than a third of community health center physician positions were filled. Pharmacists and pharmacy assistants were also hard to find-few clinics had them at all, and only about one-third of the pharmacy assistant positions posted community health centers were filled in the See Exhibit 1 for more information on the health system in South Africa. The Strategic Planning Process Ms. Julia Kekana, the Lesedi District Officer for Health Planning and Reporting, added to Mr. Nkosi's description of the strategie planning process (see Exhibit a): In April of 2011, the National Department of Health sends out their planning priorities for the 2012-13 fiscal year (FY). Fiscal years begin in April, so FY 2011-12 has just begun when the planning process for 2012-13 starts. Soon after, the Provincial Health 2 Strategie Planning in Lesedi District, South Africa PHS-001 vehicles, etc., nor are they able to eolleet the parental consent forms for every student in . each school. The senior financial manager of the sub-district chimed in on the relationship between the planning process and the budgets received: Each hospital facility develops and submits its own budget, but funding is allocated to hospitals based on whatever they got before. The submitted Hospital managers are all clinicians and don't really want to spend time understanding the budget, so they delegate to low-level staff the responsibility of developing and monitoring the budget performance Mr. Nkosi summarized the challenges Everything we ask for must be in our operational plans, which then must be captured in the strategie plan. But planning is driven by the budget, not vice versa. We get our The Performance Monitoring Process Data Collection Process at the District and Sub-district Level Lesedi District's Information Officer, Ms. Ayanda Maseko, described her role: I coordinate the health information coming in from the various sub-districts. We have a National Indicator Dataset which defines which indicators are to be collected where, and then the province adds its own set. We get data from primary health care clinics, hospitals, imaging, environmental health, the electronic TB registry, ARV (anti- retroviral) program management, ete. For instance, we collect 210 primary health care metrics and 110 hospital metrics. as there are not enough computers, and the electronic data cannot be consolidated across facilities without a ton of work. The sub-districts combine the data coming from various facilities to evaluate it, and try to put any missing information into the reports before they come to me for analysis. Program managers such as the HIV program manager and TB manager also use the data. Everything gets presented to the District management team, and I help to highlight areas that might need fixing. We then share the data at all levels of the organization. The local ram managers have to report to their sub-district managers in person on what they ve done/plan to do, etc. The Lesedi District Program Coordinator commented on the quality of the data used in the District's Performance Reports: The sub-distriets and their facilities can't possibly be doing all of what their l thhe exciusive use ord.Chang, 2017. Strategic Planning in Lesedi District, South Africa PH5-001 reports say they are doing. The original source at clinic will say a number is 4; but in the report, that number is 10. The people producing some of the raw data d hey may not understand what a "midnight census" is-a 8 s such as a "half-day patient. And there is no way to figure out what is wrong we don't have the resources to audit everything so the data is wrong every day. It often undercounts the patient load which then throws the cost estimates off. For instance, a patient sitting in an outpatient clinic all day needs food but isn't counted. Quarterly Performance Reports and Reviews Each sub-district manager reported their data to the District Manager, who, after reviewing it with the sub-district managers, produced a District-wide Department for the Provincial Health i District was required to pril, July, October, and January These reports were generally delivered in person by District Managers to the Provincial office, and their performance was reviewed with provincial leadership. The Province then combined the various District reports and submitted them to the National DOH, generally within a week after receiving the Districts' reports. Mr. Nkosi described the challenge of generating the quarterly reports and undertaking the reviews with his sub-district managers: The quarterly performance meetings with my sub-district and facility managers are not always up to the standards we wish they were. They are often used by the sub-distriet and facility managers as an opportunity to ask for more resources to offset their poor management skills. uns ate When you look below districts a programs to institutions and facilities, there is little clarity regarding what people are supposed to do. For instance, if reducing outpatient employee head count is an objective, you would expect that the hospital CEO would translate that down into the nursing executive's job description, but the linkages are not fully working. And the nursing service manager may not understand how this will impact quality of service for patients. Waiting time reduction is a goal-and there is an expectation that the facility manager will figure out ways to do that, such as having a triage person or a booking system for chronic patients. It is this level of translation, however, that does not always happen. Front-line managers, most of whom are clinicians, need training; people are in these positions in administration for reasons other than administrative skills At the provincial level, other frustrations with the planning and budgeting process emerged. As the Provincial Head of Department (HOD), explained, Department of Health lacks strategie focus We are so busy following the planning e deadlines-and we don't miss the deadlines-that we have to overwork ou this adversely affects productivity, quality of planning and service and long-term budgeting. Finally, we need to synchronize all the different reports livery. Also our trad we need short-, medium-, For the exclusive use of J. Chang, 2017. Strategic Planning in Lesedi District, South Africa PH5-001 We need to train the District Managers and the Provincial executive team to stop pushing paper. The Provincial focus is too operational. We miss the Big Picture. We should let facility managers be operational. We should expect the District Managers in areas with high HIV to ask, "What is it that we are doing wrong and what can we do about it?" And then the budget should move toward HIV, but that is not reflected in the traditional budgeting process. Looking Ahead As District Manager, Mr. Nkosi was hopeful that the future would bring increased resources and better health to his local population. It was imperative that the planning and budgeting process support a healthier future in the district. He was wondering what additional skills he needed to learn to better work the system. He also was thinking about whether the system itself might be improved, and if so, how. For the exclusive use of J. Chang, 2017. PHS-001 Strategic Planning in Lesedi District, South Africa Primary healthcare is concentrated in urban areas, so much of the rural population is without adequate access to elinics and the referral system. Much of the country's poor population, even in more urban areas, relies on traditional healers. The government is currently implementing a national health insurance scheme, and strenthening the public health system to improve access to high quality care for all. The following organizational chart gives an overview of the structure of the health system. Funds are allocated by the National Treasury to the National and Provincial Health Departments; the Provincial legislature then allocates funds to the local Districts. The allocation system is subject to political pressures at multiple points National Minister of Health (MOH) Department of Health Head of Department Provincial Health Department Provincial District Manager, District X. Mr. Nkosi Ms. Kekana Officer, Ms. Maseko Program Coordinator Sub-District ManrMarnages Sub-District Sub-District Manager Facility Health Centers For the exclusive use of J. Chang, 2017. PHs-001 Strategie Planning in Lesedj District, South Africa Exhibit 2: Planning, Budgeting Monitoring and Evaluation Processes and Time Lines 2011 2011 20111011 20112 2 2011 2012 2012 2012 Panning p oes Final am National Dept provinces and dra ram Provincia Health Dept oDisticts Final budgets DHER Provincial Oately te week Pertomance Conducted Promance Conducte Submlied to pot (PY201 Abbreviations: AG: Auditor-General DHER: District Health Expenditure Review MTEF: Medium Term Expenditure Framework NT: National Treasury This dooument is authortzed for use only by Chang in 2017 For the exclusive use of J. Chang, 2017. Strategic Planning in Lesedi District, South Africa PH5-001 Exhibit 2, continued Technical Support Month April to JuneDistrict to review Audit of previous Activities Technical review done for each year's activities (situational analysis district: together with all quarterly reports) DHER and Annual Report Review Tools: .i. District Annual Report .i. District Heath Expenditure Integrity of analysis and Integrity of data sources to be verified Review conclusions veified Confirmation of Provincial Strategic Part A: Identification of challenges Priorities and systems gaps . Prioritisation . First draft District Health Plan for the Part B September forthcoming financial year Results based planning-technical . To be based upon Annual Report and support National and Provincial Priorities First draft of the Provincial Annual Performance for the forthcoming financial year (Inputs from the DHP form the basis for the Programme 2 nputs) .Financial review and financial forecasting-using the DHER as basis-to inform the first submission of Budget statement 2 Interpretation and strategic guidance-new policy directive- .First Draft of MTEF Budget-Budgetimplications and costing Statement 2 (Inputs from the DHER Costing of plans-technical review and the DHP forms the basis for theMarginal adjustments to budgets Programme 2 input) October to National and Provincial MTEC December Hearing and targets Full technical review of District Plans and feedback . 22nd Draft District Health Plarn 2" Draft Provincial Annual Performance Plan 2" Draft Budget Statement 2 January toFinal Budget Allocation Letter Technical support for alignment of plan with confirmed budget Technical support for the operationalization of DHP March Final APP Final DHP This dooument is authorized for use orly by Ji Chang in 2017 For the exclusive use of J. Chang, 2017. Strategic Planning in Lesedi District, South Africa PHs-001 Exhibit 3: National Health Systems Priorities for 2010-2015 Sample District Activities 2015 Facilitate career exhibitions on 2015 Target 85 schools National Priority Provision of Strategic Leadership and Creation of Social Compact for Better Health Outcomes health at high schools Recruit students to study medicine in 7 students Cuba Facilitate access to internal bursary 115 students Conduct Primary Health Care I implement NH Master Plan 16 campaigns Implementation of National Health Insurance Improve the Quality of Heath Assess the implementation of Quality 12 hospitals &10 Services Improvement Plans CHCs Facilitate implementation of Quality Assurance Program Facilitate the reduction of the vacancy rate for critical and scarce skills 160 programs Reduce from 58% to | 45% Train Community Health Workers on 324 workers Reengineering of PHC Revitalization of Infrastructure Urgent implementation of refurbishment and maintenance of district hospitals, CHCs, and Clinics 162 facilities Accelerated Implementation of Implement adult and paediatric HIVIAIDS strategic plan and treatment guidelines at al PHC increased focus on TB and other communicable diseases Mass mobilization for the better health of the population Place more focus on programs to facilities Intensify health promotion programs 16 programs attain Millennium Development Goals Conduct awareness campaigns on diseases of Ifestyle No related District activities Commission research to accurately quantify maternal and infant mortality Commission research on the impact of social determinants of health Review of Drug Policy Strengthen research and For the exclusive use of J. Chang, 2017. PIIs-00r Strategie Planning in Lesedi District, South Africa Exhibit 4: Sample of District Health Plan for Primary Health Care Strategie Goal o1: To facilitate a functional quality-driven primary health care system that provides an integrated and seamless package of health needs, services and is responsive to eustomer Strategic Challenges: Underutilization of PHC due to bad roads, small facilities; poor drug management at all levels; shortage of personnel, inadequate professional skills; poor maintenance systems; lack of sustainable transport; and poor data quality. Measures of Performance: 10 measures of vacancy rates for skilled professionals (doctors, nurses, pharmacists) 5 measures of vacancy rates for other human resource categories at primary health care facilities 15 measures of patient head count, utilization rates, expenditures per head count, and clinical workload per professional nurse and doctor, and facility supervisory visits Exhibit 5: Budget of Lesedi District, 2011-2012 Values in SA Rand Sub Program Provincial Budget %Over Variation from Appropriation Expenditure (Under) Spent Prior Year in Real Terms (5%) 100,247,478 341,030,680 (10%) (3%) 1 10% 90,015,661 330,803,880 District Management Community Health Other Community HMIAIDS 34252.021147380418 25% (68%) 126% 51% 18% 13% 14% 6% 461,663 82,348.286 9,855,834 490,756 71,321,205 (13%) 8,127,845| (18%)| 1 654.864.794 640,198.83 Subtotal: Primary Health Services District Hospitals Total Lesedi District (2%) 12% 3% 616,630,662 689,110.193 1,371,742,934 1,419,322,689 Thie document is authorized lor use orly by Chang in 2017