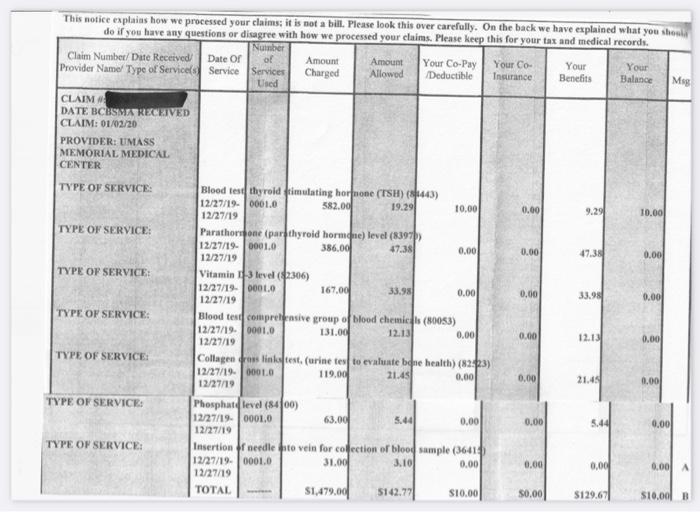
The attached file reflects an actual insurance statement of bloodwork performed for an outpatient visit. Take note of the following total costs: Total amount charged by the hospital laboratory Total amount allowed by the insurance company Total amount owed by the patient In light of our previous discussions about the high cost of healthcare here in the U.S., how does: The hospital laboratory rationalize the total amount charged? The insurance company reduce the total amount allowed by roughly 90.4%? Any of this make sense? M This notice explains how we processed your claims: it is not a bill. Please look this over carefully. On the back we have explained what you should de if you have any questions or disagree with how we processed your claims. Please keep this for your tax and medical records. Number Claim Number/ Dute Received Date of of Amount Amount Your Co-Pay Your Co- Your Your Provider Name Type of Service Service Services Charged Allowod Deductible Insurance Benefits Balance Used CLAIM DATE BCBS RECEIVED CLAIM: 01/02/20 PROVIDER: UMASS MEMORIAL MEDICAL CENTER TYPE OF SERVICE: Bloed te thyroid ftimulating hormone (TSH) (443) 12/27/19.0001.0 582.00 19.291 10.00 0.00 9.29 10.00 12/27/19 TYPE OF SERVICE: Parathoone (par thyroid hormone) level (8397 12/27/19.00010 386.00 47.381 0.00 0.00 0.00 12/27/19 TYPE OF SERVICE Vitamin D-3 level (2306) 12/27/19.00010 167.00 33.98 0.00 0.00 33.98 0.00 12/27/19 TYPE OF SERVICE: Blood tes comprehensive group of blood chemics (80053) 12/27/19.0001.0 131.00 0.00 0.00 12.13 0.00 12/27/19 TYPE OF SERVICE Collagen crosslinktest. (urine testo evaluate que health) (2:3) 12/27/19.000LO 119.00 21.45 0.00 0.00 21.481 0.00 12/27/19 TYPE OF SERVICE: Phosphat level (8400) 12/27/19.00010 63.00 5.44 0.00 0.00 5.44 0,00 12/27/19 TYPE OF SERVICE: Insertion needle to vein for collection of blood sample (36414 12/27/19.0001.0 31.00 3.10 0.00 0.00 0.00 0.00 12/27/19 TOTAL 51,479.00 5142.77 SI0.00 50.00 $129.67 S10.00 12.13 The attached file reflects an actual insurance statement of bloodwork performed for an outpatient visit. Take note of the following total costs: Total amount charged by the hospital laboratory Total amount allowed by the insurance company Total amount owed by the patient In light of our previous discussions about the high cost of healthcare here in the U.S., how does: The hospital laboratory rationalize the total amount charged? The insurance company reduce the total amount allowed by roughly 90.4%? Any of this make sense? M This notice explains how we processed your claims: it is not a bill. Please look this over carefully. On the back we have explained what you should de if you have any questions or disagree with how we processed your claims. Please keep this for your tax and medical records. Number Claim Number/ Dute Received Date of of Amount Amount Your Co-Pay Your Co- Your Your Provider Name Type of Service Service Services Charged Allowod Deductible Insurance Benefits Balance Used CLAIM DATE BCBS RECEIVED CLAIM: 01/02/20 PROVIDER: UMASS MEMORIAL MEDICAL CENTER TYPE OF SERVICE: Bloed te thyroid ftimulating hormone (TSH) (443) 12/27/19.0001.0 582.00 19.291 10.00 0.00 9.29 10.00 12/27/19 TYPE OF SERVICE: Parathoone (par thyroid hormone) level (8397 12/27/19.00010 386.00 47.381 0.00 0.00 0.00 12/27/19 TYPE OF SERVICE Vitamin D-3 level (2306) 12/27/19.00010 167.00 33.98 0.00 0.00 33.98 0.00 12/27/19 TYPE OF SERVICE: Blood tes comprehensive group of blood chemics (80053) 12/27/19.0001.0 131.00 0.00 0.00 12.13 0.00 12/27/19 TYPE OF SERVICE Collagen crosslinktest. (urine testo evaluate que health) (2:3) 12/27/19.000LO 119.00 21.45 0.00 0.00 21.481 0.00 12/27/19 TYPE OF SERVICE: Phosphat level (8400) 12/27/19.00010 63.00 5.44 0.00 0.00 5.44 0,00 12/27/19 TYPE OF SERVICE: Insertion needle to vein for collection of blood sample (36414 12/27/19.0001.0 31.00 3.10 0.00 0.00 0.00 0.00 12/27/19 TOTAL 51,479.00 5142.77 SI0.00 50.00 $129.67 S10.00 12.13