

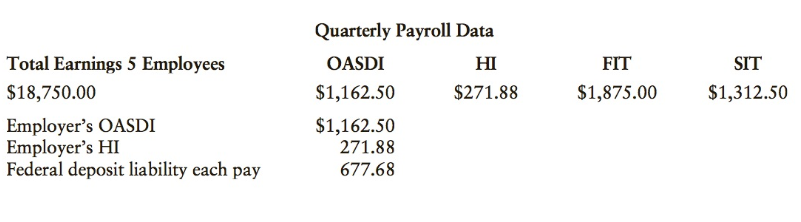
During the fourth quarter of 2017, there were seven biweekly paydays on Friday (October 6, 20; November
Question:
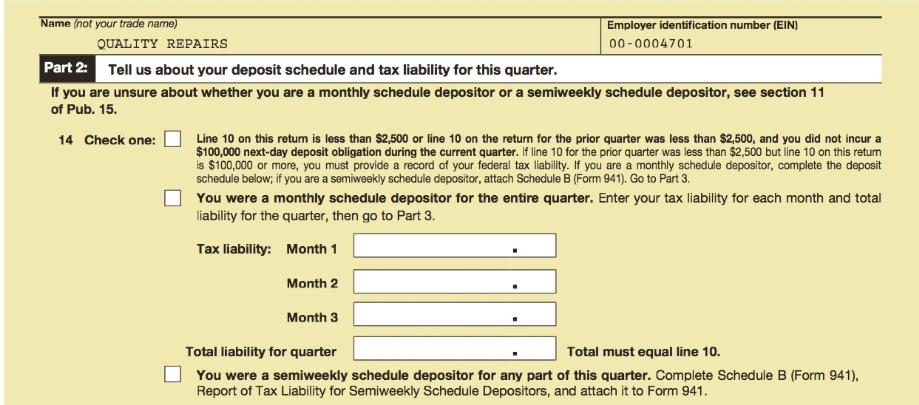
a. Complete the Federal Deposit Information Worksheets reflecting electronic deposits (monthly depositor). The employer€™s phone number is (501) 555-7331. Federal deposit liability each pay, $677.68.
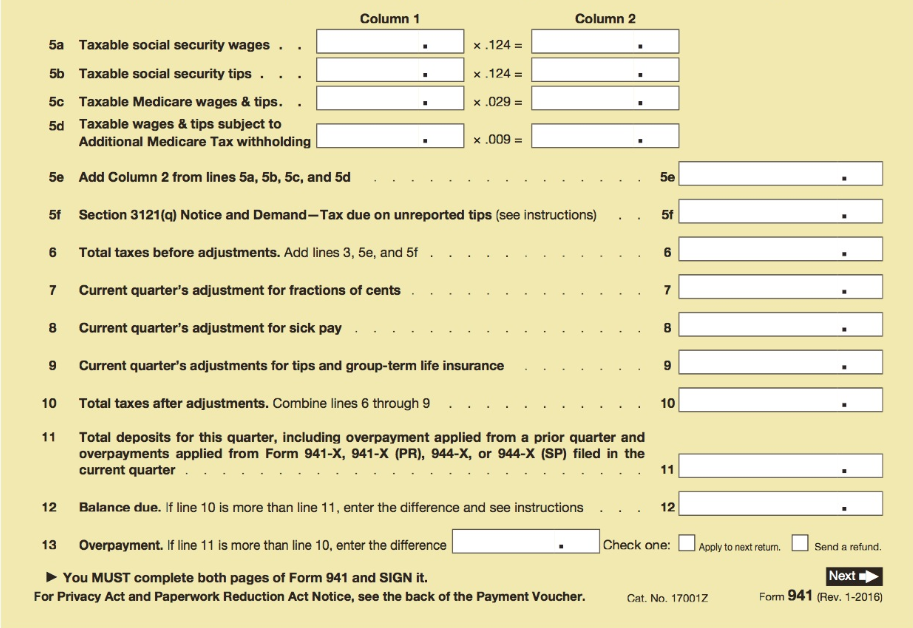
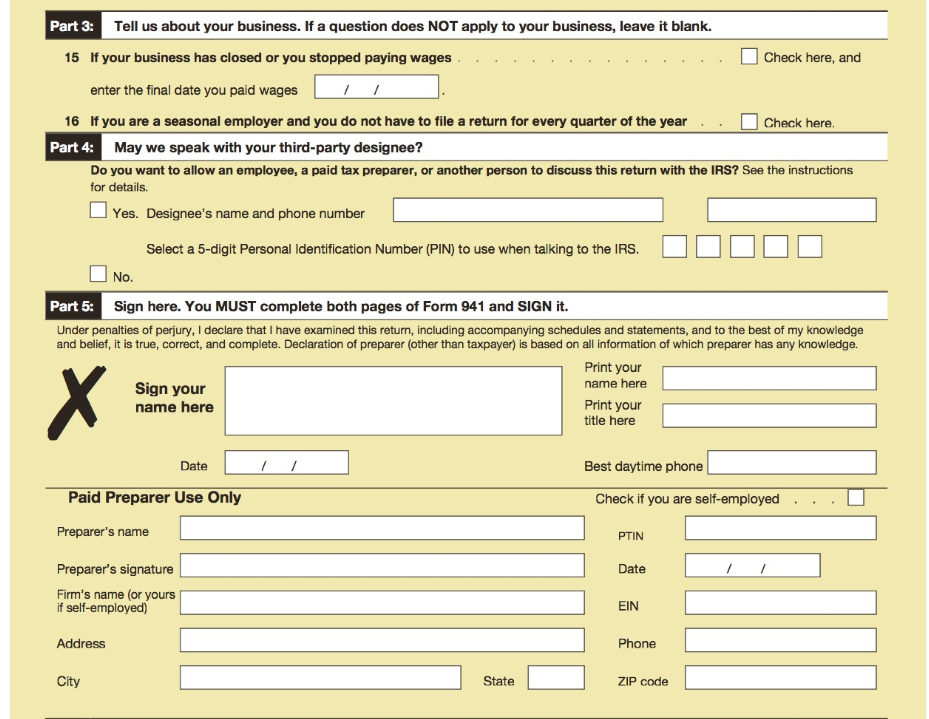
b. Employer€™s Quarterly Federal Tax Return, Form 941. The form is signed by you as president on January 31, 2018.
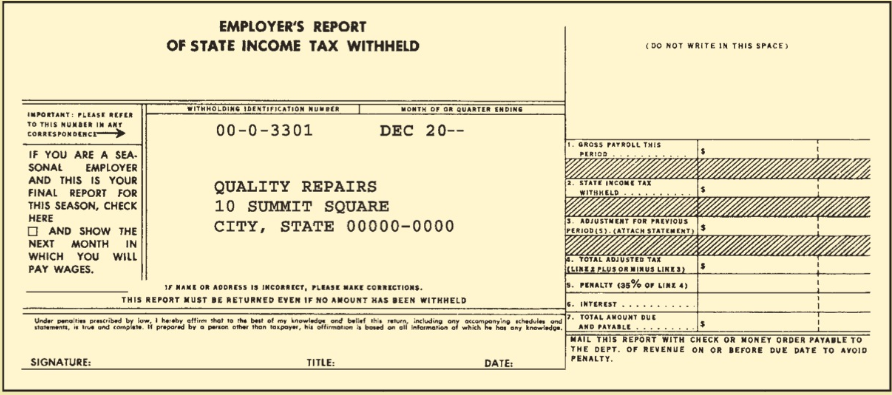
c. Employer€™s Report of State Income Tax Withheld for the quarter, due on or before January 31, 2018.
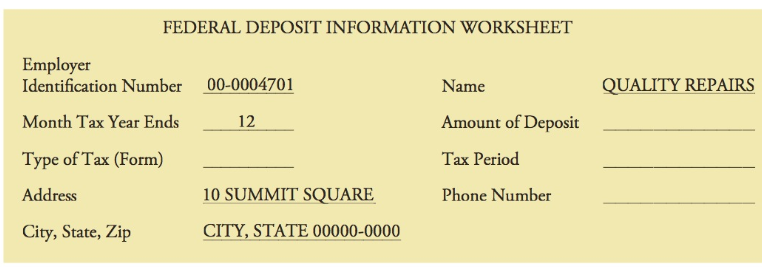
To be deposited on or before _____________
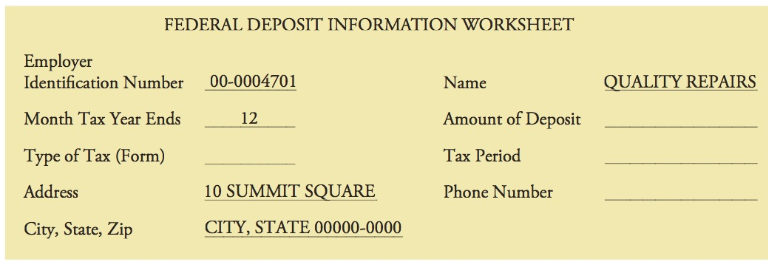
To be deposited on or before ______________
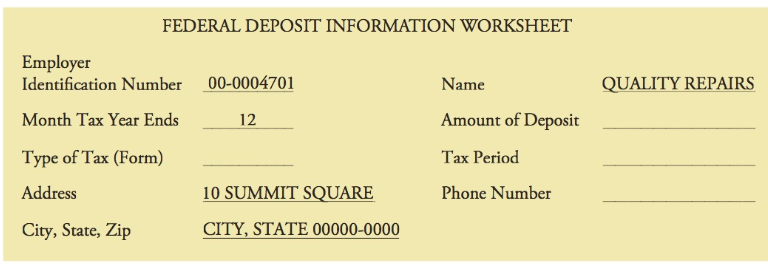
To be deposited on or before ______________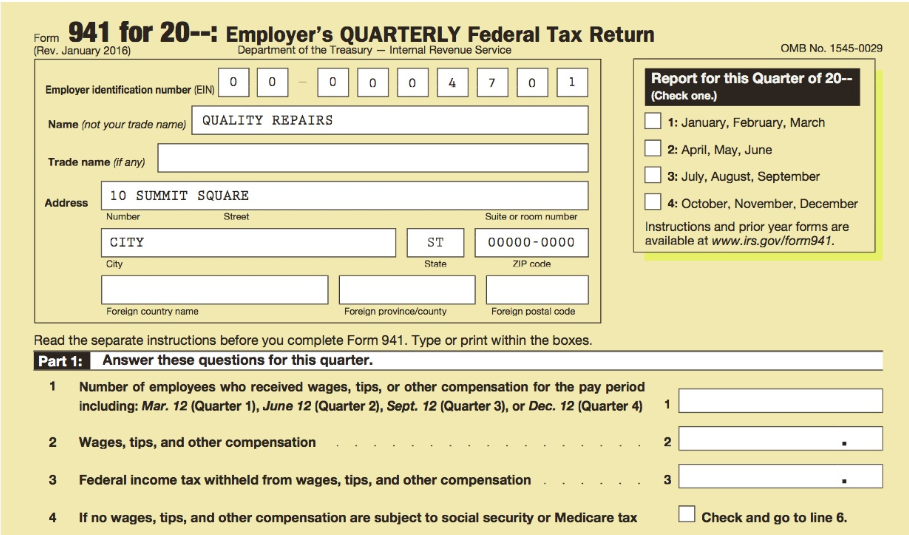
Fantastic news! We've Found the answer you've been seeking!
Step by Step Answer:
a To be deposited on or before November 15 2017 To be deposited on or befo...View the full answer

Answered By
Bhartendu Goyal
Professional, Experienced, and Expert tutor who will provide speedy and to-the-point solutions. I have been teaching students for 5 years now in different subjects and it's truly been one of the most rewarding experiences of my life. I have also done one-to-one tutoring with 100+ students and help them achieve great subject knowledge. I have expertise in computer subjects like C++, C, Java, and Python programming and other computer Science related fields. Many of my student's parents message me that your lessons improved their children's grades and this is the best only thing you want as a tea...
2+ Reviews
10+ Question Solved
Related Book For 
Question Posted:
